Many veterans know their own monthly disability compensation amount down to the dollar. Far fewer know what that number looks like at scale — how much the VA pays out in total, where that money concentrates, and how quickly it’s growing. The FY2025 VBA Compensation Report puts real numbers behind those questions, and the picture it paints is bigger and more concentrated than most people assume.
But why does it matter?
Understanding where VA disability dollars go (which VA rating levels absorb most of the budget, which states receive the most, and how fast the system is growing) helps you calibrate your own expectations and strategy.
If most of the money is flowing to veterans with a 100% VA rating, that tells you something about where the VA’s own resources and attention are concentrated, and where the gap between a partial rating and a full one really matters financially.
This article breaks down the numbers: the national total, how VA disability compensation is distributed by rating tier, what the data shows about state-level totals, and what it means for your own claim strategy.
Table of Contents
Summary of Key Points
The VA paid $174.05 billion in disability compensation to 6,338,253 veterans in FY2025 (an average of $27,461 per veteran).
Veterans rated 100% disabled received $93.8 billion, or 53.9% of the entire compensation budget, despite being under 30% of all recipients.
Total compensation grew 5.8% year-over-year as the veteran population on the rolls grew from 5,992,967 to 6,338,253.
Florida received $13.1 billion in annual VA disability compensation in the most recent state-level data (more than any other state), with Texas, California, North Carolina, and Virginia rounding out the top five.
Dependency and Indemnity Compensation (DIC) for surviving families added another $11.51 billion on top of veteran compensation, reaching 549,324 recipients.
In FY2025, the VA paid $174.05 billion in disability compensation to 6,338,253 veterans (an average of $27,461 per veteran for the year). Veterans rated 100% disabled made up less than a third of all recipients but received $93.8 billion of that total, or 53.9% of every dollar the VA paid out. Florida alone accounted for $13.1 billion in annual compensation, more than any other state.
-VA Claims Insider
How Much the VA Actually Pays Veterans
As of September 30, 2025, the VA was paying disability compensation to 6,338,253 veterans nationwide, a total of $174.05 billion for the fiscal year. That works out to an average of $27,461 per veteran annually — roughly $2,288 a month, though individual payments vary widely based on rating percentage and number of dependents.
That total isn’t static. The compensation rolls grew by 345,286 veterans compared to FY2024 (a 5.8% increase), while 476,802 veterans filed as new recipients during the year. The dollar total is growing even faster than the recipient count, for a straightforward reason: the veterans joining the rolls, and the veterans already on them, are accumulating more service-connected disabilities and moving toward higher combined ratings over time.
Where the Money Concentrates: The Rating-Tier Breakdown
The single biggest driver of the FY2025 compensation total is the 100% disability tier. Veterans rated 100% received $93.8 billion of the $174.05 billion paid out — 53.9% of the entire budget — even though they represent well under a third of all recipients. Put another way: the remaining $80.2 billion (46.1% of the budget) is spread across every veteran rated anywhere from 10% through 90%.
That concentration is intensifying, not stable. The table below shows how the recipient count at each rating tier changed between FY2024 and FY2025. Every tier from 70% and above grew. Every tier from 30% and below shrank.
Rating
FY2024 Recipients
FY2025 Recipients
YoY Change
100%
1,547,842
1,847,449
+299,607 (+19.4%)
90%
621,930
679,688
+57,758 (+9.3%)
80%
595,721
627,300
+31,579 (+5.3%)
70%
545,452
562,930
+17,478 (+3.2%)
30%
335,731
320,674
-15,057 (-4.5%)
20%
371,767
355,239
-16,528 (-4.4%)
10%
877,391
861,702
-15,689 (-1.8%)
Source: FY2025 VBA Compensation Report, five-year rating distribution tables. The 40%–60% tiers are omitted here because the underlying report did not publish complete year-over-year recipient counts for those levels; the report does note that 40% ratings declined 2.5% year-over-year, consistent with the broader pattern above.
Which States Get the Most
The most recent data shows a clear leader in state-level veterans benefits: Florida veterans received $13.1 billion in annual disability compensation, more than any other state. Texas, California, North Carolina, and Virginia round out the top five states by total compensation volume.
That ranking tracks with veteran population size and cost of living more than with any state-specific VA policy — Florida, Texas, and California are simply home to large numbers of veterans, many of them retirees who relocated after service. If you’re comparing your own state’s veteran benefits landscape, this compensation ranking is a useful companion to our guide to the best veteran benefits by state, which covers the state-level programs — property tax exemptions, tuition waivers, and similar — that stack on top of federal compensation.
The $174.05 billion in veteran compensation doesn’t include Dependency and Indemnity Compensation (DIC) — the separate benefit paid to surviving spouses, children, and dependent parents of veterans who died from service-connected conditions. DIC added another $11.51 billion in FY2025, reaching 549,324 recipients nationwide. New DIC claims are growing faster than veteran compensation itself — a trend significant enough to warrant its own look at what’s driving it.
Two forces are pushing the total budget higher year over year: more veterans are joining the compensation rolls (up 5.8%), and the veterans already on the rolls are accumulating more service-connected disabilities and moving into higher rating tiers.
Total service-connected disabilities on file grew 11.6% in FY2025 — nearly double the rate at which the veteran population itself grew. That gap between “more veterans” and “more disabilities per veteran” is the real engine behind the rising dollar total, and it’s worth understanding on its own terms.
What This Means for Your Claim
These numbers aren’t just background context — they’re a rough map of where the VA’s compensation system rewards precision. The jump from 90% to 100% is worth more to your household budget than any other single step in the rating scale, which is exactly why that tier shows the steepest year-over-year growth.
If your combined rating has been sitting in the 70%–90% range for a while, the most direct paths forward may be the ones already available in your claim file: previously unrated secondary conditions, or a condition that has worsened enough to justify a VA rating increase.
PRO TIP: Easily see what an increase could do to your monthly compensation with our VA Disability Calculator.
Conclusion
The VA’s $174.05 billion disability compensation system is larger, faster-growing, and more concentrated at the top of the rating scale than most veterans realize. Over half of every dollar paid out goes to the roughly one-in-four veterans who have a 100% VA rating, and that concentration grew sharply in FY2025. Whether you’re evaluating your own claim strategy or just trying to understand the system you’re part of, the rating tier you’re sitting at matters more to the math than almost anything else in your file.
YOU SERVED. YOU DESERVE.
You served. You earned the right to file. You earned the right to be heard. And you earned the right to pursue every VA benefit you legally qualify for.
So here is the real question:
Do you have the VA rating you were given, or the VA rating you truly deserve?
Want Expert-Level VA Claim Help? WE GOT YOUR SIX!
VA Claims Insider helps educate and empower veterans to get the VA rating they deserve.
Work directly with a VA Claims Insider Coach who can help lead you to VA claim victory.
50,000+ disabled veterans served in our membership programs since 2016.
33% average rating increase for veterans who complete our Elite program.
How much does the VA pay veterans in disability compensation each year?
In FY2025, the VA paid $174.05 billion in disability compensation to 6,338,253 veterans nationwide, an average of $27,461 per veteran for the year.
What’s the average VA disability payment per veteran?
The FY2025 average was $27,461 per year, or roughly $2,288 per month. Individual payments vary significantly based on your combined rating percentage and the number of dependents on your award.
Which states receive the most VA disability compensation?
Florida leads with $13.1 billion in annual compensation, followed by Texas, California, North Carolina, and Virginia, according to the VA’s most recent state-level data.
Why do veterans rated 100% receive over half of all VA compensation?
Veterans at 100% receive the maximum monthly rate, and the FY2025 data shows this group grew 19.4% year-over-year — far faster than any other rating tier. That combination of the highest per-veteran payment and the fastest-growing group is why 100%-rated veterans account for 53.9% of the entire compensation budget.
Is VA disability compensation taxable?
No. VA disability compensation is not subject to federal income tax, regardless of your rating percentage. For a full explanation of how this affects other benefits and tax filings, see VACI’s guide to whether VA disability is taxable.
How is my monthly VA disability payment amount determined?
Your payment is based on your combined disability rating and the number of dependents (spouse, children, dependent parents) on your award. The VA publishes updated payment charts each year — see the 2026 VA disability pay chart for exact monthly amounts by rating and dependent status.
About the Author
Eric Webb
Eric has written and worked in the field of Veterans Disability since 2020 and enjoys writing educational content for the veteran population. His prior work has been published in the Official Journal of the American College of Sports Medicine (ACSM). He holds a Degree in Health and Exercise Science.
According to the Veterans Benefits Administration Annual Benefits Report for Fiscal Year 2025, nearly 1.85 million veterans now receive compensation at the 100% disability level. That’s an increase of 299,607 veterans, or 19.4%, in just one year. Today, almost 3 out of every 10 veterans receiving VA compensation have a 100% VA disability rating.
That doesn’t mean the VA has lowered its standards or that getting a 100% rating is easy, but it does suggest something important has changed.
Over the past several years, more veterans have become aware of the benefits they’ve earned. The PACT Act expanded eligibility for many toxic exposure claims, and more veterans are pursuing secondary service connection, requesting rating increases when disabilities worsen, and submitting stronger medical evidence.
Whether you’re filing your first claim or wondering if your current VA disability rating still reflects your health today, understanding these trends can help you make more informed decisions about your own benefits.
Summary of Key Points
Nearly 1.85 million veterans now receive a 100% VA disability rating, an increase of 299,607 veterans (19.4%) compared to the previous year.
Veterans rated at 100% now make up more than 29% of everyone receiving VA disability compensation, making it the largest combined disability rating category.
The growth reflects several long-term trends, including expanded eligibility through the PACT Act, more secondary service connection claims, and veterans seeking increases as service-connected conditions worsen over time.
While more veterans are receiving 100% ratings, the legal standards for disability ratings haven’t changed. Strong medical evidence and documentation remain the foundation of every successful claim.
Table of Contents
The Myth of the “Impossible” 100% Rating
For many veterans, the idea of receiving a 100% VA disability rating felt out of reach.
Some assumed it was reserved only for catastrophic combat injuries or those with a single, life-changing disability.
The latest VBA data challenges that perception.
Today, 1,847,449 veterans receive compensation at the 100% level, making it the largest combined disability rating category in the entire VA compensation system.
That’s a remarkable change, and it didn’t happen because of relaxed VA standards. Compared to even 10 years ago, today’s disability system looks very different.
More veterans are filing claims.
More veterans are identifying secondary conditions.
More veterans qualify under expanded presumptive rules.
More veterans are seeking increases when their service-connected disabilities worsen over time.
The result is a disability system where reaching a 100% schedular rating is no longer the rare exception many people once believed it to be.
A 100% Rating Doesn’t Usually Mean One Severe Disability
Another common misconception is that every veteran with a 100% rating has one catastrophic injury.
In reality, many veterans reach a schedular 100% rating through a combination of multiple service-connected conditions.
For example, someone might have service-connected:
Individually, none of those conditions may be rated at 100%, but when the VA combines disability ratings using its unique formula, often called “VA math,” the combined evaluation can reach 100%.
Understanding how combined ratings work is important because many veterans underestimate how close they already are to reaching the next rating level.
Pro Tip: Quickly calculate your monthly VA disability compensation with our easy-to-use VA Disability Calculator.
100% VA Disability Statistics: 100% Now the Largest Disability Rating Category
One of the most surprising findings in the VBA report is how the number of veterans receiving a 100% rating compares to every other combined disability rating.
Today, there are significantly more veterans rated 100% than there are at 90%, 80%, or 70%.
Combined VA Disability Rating
Veterans Receiving Compensation
100%
1,847,449
90%
679,688
80%
627,300
70%
562,930
60%
450,286
That makes the 100% category the single largest combined disability rating in the VA compensation system.
This wasn’t always the case.
As awareness of VA benefits has grown, and as more veterans have developed additional service-connected conditions over time, the distribution of disability ratings has changed dramatically.
Why Are More Veterans Receiving a 100% VA Disability Rating?
Rather than one major policy change, the increase in 100% ratings is likely the result of multiple factors.
Let’s take a closer look at a few of the biggest:
1. The PACT Act Expanded Eligibility for Millions of Veterans
The law expanded eligibility for many veterans exposed to toxic substances during military service by adding new presumptive conditions and broadening recognition of toxic exposure.
For many veterans, that meant finally receiving service connection for conditions that had previously been denied or difficult to prove.
Once service connection is established, additional secondary conditions may also become eligible for compensation if they’re medically linked to the primary disability.
The result is a growing number of veterans entering or re-entering the disability compensation system.
2. Veterans Are Identifying More Secondary Service-Connected Conditions
Another major shift is education.
Twenty years ago, many veterans filed claims only for the injuries they experienced while serving.
Today, there’s greater awareness that service-connected disabilities can lead to additional medical conditions later in life.
For example, a veteran with a service-connected knee injury may later develop hip problems or chronic back pain because of altered gait mechanics.
Someone living with PTSD may also develop depression, anxiety, sleep disturbances, migraines, or gastrointestinal issues.
Those secondary conditions can be compensable when supported by medical evidence and a nexus connecting them to an existing service-connected disability.
3. Service-Connected Disabilities Often Get Worse Over Time
Another reason more veterans are reaching a 100% VA disability rating is simply the reality of aging with service-connected disabilities.
Many conditions naturally progress over time. What started as manageable pain or mild symptoms during your military service may become significantly more limiting years later.
For example, it’s common for veterans to experience worsening:
Personal lay statements explaining how symptoms affect work and daily life
None of these guarantees approval, but they paint a more complete picture of how your service-connected conditions affect your life.
Does This Mean It’s Easier to Get a 100% VA Disability Rating Today?
No. The legal standards used to assign disability ratings haven’t suddenly become more lenient.
The VA still evaluates disabilities using the Schedule for Rating Disabilities (38 CFR Part 4), just as it has for decades.
So why are so many more veterans reaching 100%? Today, veterans often have:
Greater awareness of their earned benefits
More complete medical documentation
Additional secondary service-connected conditions
Expanded eligibility through laws like the PACT Act
Disabilities that have progressed over time
In other words, more veterans are qualifying because they meet the existing requirements, not because the requirements have changed. And that’s an important distinction.
What These Trends Could Mean for Your Own VA Disability Claim
The numbers in the VBA report are interesting, but what do they mean for your own situation?
While you may not be pursuing a 100% rating, your disability rating should accurately reflect the severity of your service-connected conditions today.
Here are a few questions worth asking yourself:
Have your service-connected conditions worsened since your last VA rating decision?
Have you developed new conditions that may be secondary to an existing service-connected disability?
Are all your current symptoms documented in your medical records?
Do you understand how the VA combines disability ratings?
If you answered “yes” to any of those questions (or “no” to the last one), it may be worth reviewing your current disability ratings and the evidence supporting them.
Your biggest opportunity could be making sure your existing claims accurately reflect your current level of disability.
Don’t Compare Your Rating to Someone Else’s
The surge in 100% ratings doesn’t mean everyone has the same path.
Two veterans with the same diagnosis may receive different ratings because of differences in:
Symptom severity
Medical evidence
Functional impairment
Applicable diagnostic codes
Instead of comparing your rating to someone else’s, focus on building the strongest evidence for your own.
Conclusion
The biggest takeaway from the FY2025 VBA Annual Benefits Report is that old assumptions about who qualifies for a high disability rating no longer tell the whole story.
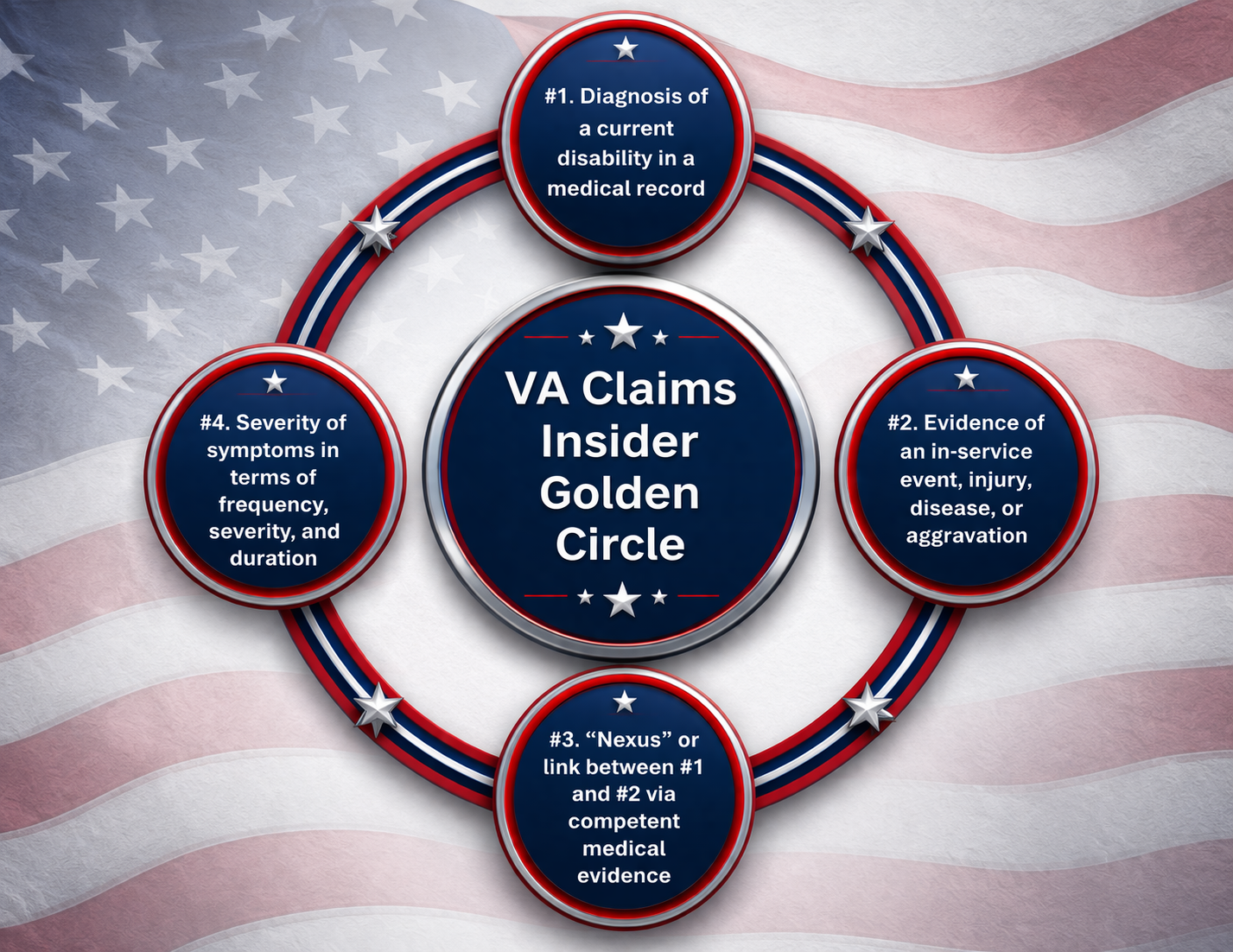
The VA hasn’t changed its disability policies. It still requires veterans to provide a current diagnosis of a condition, evidence of an in-service event, and strong medical evidence and documentation that support the rating criteria and service connection.
What has changed is that more veterans are understanding the claims process, documenting secondary conditions, seeking increases when disabilities worsen, and taking advantage of expanded eligibility under laws like the PACT Act.
If you thought a 100% VA rating was out of reach, the latest data is a reminder that every claim deserves to be evaluated on its own merits.
While the goal isn’t to chase a certain percentage, it’s important that your VA disability rating accurately reflects how your service-connected conditions affect your life today.
YOU SERVED. YOU DESERVE.
You served. You earned the right to file. You earned the right to be heard. And you earned the right to pursue every VA benefit you legally qualify for.
So here is the real question:
Do you have the VA rating you were given, or the VA rating you truly deserve?
Want Expert-Level VA Claim Help? WE GOT YOUR SIX!
VA Claims Insider helps educate and empower veterans to get the VA rating they deserve.
Work directly with a VA Claims Insider Coach who can help lead you to VA claim victory.
50,000+ disabled veterans served in our membership programs since 2016.
33% average rating increase for veterans who complete our #1 rated Elite program.
How many veterans have a 100% VA disability rating?
1,847,449 veterans receive compensation at the 100% disability level. That’s nearly 29.2% of everyone receiving VA disability compensation.
Why did the number of 100% VA disability ratings increase so much?
The VBA report doesn’t identify one specific cause, but several long-term trends likely contributed, including implementation of the PACT Act, expanded presumptive conditions, more secondary service connection claims, stronger medical evidence, and disabilities worsening over time.
Does the increase mean it’s easier to get a 100% VA disability rating?
No. The VA still evaluates disabilities under the same legal rating criteria. More veterans are reaching 100% because they’re meeting those criteria, not because the standards have been lowered.
Can you reach a 100% rating with multiple disabilities?
Yes. Many veterans receive a schedular 100% rating through a combination of service-connected disabilities rather than a single condition. The VA combines disability ratings using its own formula, often called “VA math.”
You can quickly calculate your monthly VA disability compensation with our easy-to-use VA Disability Calculator.
Can secondary conditions help you reach a 100% disability rating?
Yes. If a medical condition is caused or aggravated by an existing service-connected disability, it may qualify for secondary service connection. Additional compensable conditions can increase your combined disability rating when supported by medical evidence.
Should I apply for a rating increase if my condition has worsened?
If your service-connected disability has become more severe since your last rating decision, you may be eligible to request a VA rating increase. The VA will evaluate updated medical evidence to determine whether your current symptoms meet the criteria for a higher rating.
About the Author
Katie McCarthy
Katie McCarthy is a writer and editor with experience in daily news and digital and print magazine publishing. She honed her editorial (and firearms) skills at Guns & Ammo before helping launch Black Rifle Coffee Company’s Coffee or Die Magazine as the managing editor. She holds degrees in English (BA) and public administration (MPA). Katie is a military spouse and word nerd who enjoys reading, hiking, camping, gardening, and spending time with her family.
BLUF: A TERA concession helps your VA disability claim, but it doesn’t automatically win it.
Many veterans are surprised to learn that a Toxic Exposure Risk Activity (TERA) concession does not guarantee service connection or VA disability benefits.
While a TERA concession is a favorable finding that acknowledges your exposure to potentially harmful substances during military service, it only satisfies one part of the service-connection equation. The VA still requires evidence of a current diagnosis and a medical nexus linking your condition to that exposure.
As a result, you may receive a decision letter stating that participation in a TERA was conceded, yet your claim is still denied.
Understanding why it happens and what evidence the VA needs can help you build a stronger claim.
Summary of Key Points
A TERA concession confirms exposure to a toxic substance or risk activity during military service.
A TERA concession does not automatically establish service connection.
Veterans must still have a current diagnosed condition and a nexus between the condition and the toxic exposure.
Many TERA-related claims are denied because the VA determines the medical evidence does not support a connection.
Additional medical evidence, including nexus letters and independent medical opinions, may help strengthen a denied claim.
Table of Contents
What is a TERA Concession?
A TERA concession is a favorable finding by the VA that acknowledges a veteran was exposed to potentially hazardous substances, environments, or activities during military service.
When the VA concedes a TERA, it means the agency accepts that the exposure occurred based on military records, service locations, occupational duties, or other evidence.
It makes sense that veterans might interpret this favorable finding as proof that the claim should be approved. Unfortunately, that’s not how the VA disability system works.
TERA Concession vs. Presumptive Service Connection
One of the biggest sources of confusion among veterans is the difference between a TERA concession and presumptive service connection.
Although both can strengthen a VA disability claim, they’re not the same.
A TERA concession acknowledges that you were exposed to a qualifying toxic substance or hazardous environment during military service.
Presumptive service connection goes a step further by allowing the VA to presume that certain conditions are related to service when specific eligibility requirements are met.
Factor
TERA Concession
Presumptive Service Connection
What it establishes
Exposure occurred during military service
Exposure and nexus are generally presumed
Favorable finding?
Yes
Yes
Must prove current diagnosis?
Yes
Yes
Must prove toxic exposure occurred?
Usually no
Usually no
Must prove medical nexus?
Often yes
Usually no
Can VA still deny the claim?
Yes
Yes, if eligibility requirements aren’t met
Applies to all conditions?
No
No
Strength of evidence provided
Moderate
Strong
Automatically results in service connection?
No
Not necessarily but improves the likelihood
Why This Difference Matters
A TERA concession is like the VA saying, “We agree you were exposed.”
Presumptive service connection is like the VA saying, “We agree you were exposed, and for this specific condition, we’ll generally presume the exposure caused it.”
That’s a significant distinction.
For example, a veteran may receive a TERA concession for burn pit exposure but still need medical evidence linking that exposure to sleep apnea, hypertension, or another non-presumptive condition.
Conversely, if a veteran develops a condition that qualifies for presumptive service connection under applicable toxic exposure laws, the nexus requirement may be substantially reduced or eliminated.
Pro Tip for Veterans
When reviewing a VA decision letter, look carefully at the favorable findings section.
Ask yourself:
Did the VA concede exposure?
Did the VA concede a diagnosis?
Did the VA concede service connection?
What element of the claim is still missing?
In many denied TERA claims, the missing piece is not exposure but the medical nexus.
One of the most common misconceptions is that a favorable finding automatically leads to service connection.
In reality, a favorable finding simply means the VA accepts a specific fact without requiring further proof.
For example, if a rating decision states, “Participation in a Toxic Exposure Risk Activity has been conceded,” that statement only confirms the exposure occurred.
It doesn’t mean the VA agrees that:
The exposure caused your condition
Your diagnosis is related to military service
Service connection has been established
A favorable finding is valuable because it removes one evidentiary hurdle, but additional evidence is often required.
The Three Elements Required for Service Connection
To understand why TERA claims can still be denied, it helps to understand the three elements generally required for service connection.
1. A current diagnosis — You must have a current diagnosis of a VA recognized or medical condition. Without a current diagnosis, your claim may be denied regardless of toxic exposure.
2. An in-service event, injury, illness, or exposure — This is where a TERA concession helps. The concession establishes that a qualifying toxic exposure occurred during military service. For many veterans, this eliminates the need to prove the exposure independently.
3. A medical nexus — The nexus is often where TERA claims succeed or fail. A nexus is medical evidence showing that the current condition is “at least as likely as not” related to military service or toxic exposure.
Even when exposure is conceded, the VA may deny the claim if it determines the evidence does not support a causal relationship.
Why the Nexus Opinion Still Matters
The nexus requirement is frequently the deciding factor in toxic exposure claims.
A veteran may have a current diagnosis, a conceded TERA exposure, and extensive treatment records, but still receive a denial.
Why?
Because the VA may conclude that the medical evidence doesn’t establish a connection between the diagnosed condition and the toxic exposure.
In many cases, VA examiners cite factors such as:
Lack of supporting medical literature
Alternative risk factors
Age-related conditions
Family history
Occupational exposures after service
When this occurs, the claim may be denied despite the TERA concession.
Common Reasons TERA Claims Get Denied
The Condition Is Not Presumptive
Some conditions qualify for presumptive service connection under specific laws and regulations, and others don’t.
If your condition isn’t presumptive, you generally need to establish the nexus (link) with medical evidence.
Negative VA Medical Opinion
A compensation and pension (C&P) examiner may conclude that the condition is “less likely than not” related to toxic exposure.
The VA often relies heavily on these opinions while making determinations.
Insufficient Medical Evidence
Claims may be denied when treatment records, medical studies, or physician opinions don’t support a connection.
Alternative Causes Identified
The VA may determine that another factor is more likely responsible for the condition than military toxic exposure.
No Current Diagnosis
Even with documented exposure, service connection generally requires a current diagnosed disability.
How to Strengthen a Denied TERA Claim
If your claim was denied despite a TERA concession, additional evidence may improve your chances upon appeal or supplemental review.
Potential evidence may include:
Independent Medical Opinions: An independent medical opinion can address deficiencies in the VA’s rationale and explain why toxic exposure likely contributed to the condition.
Nexus Letters: A strong nexus letter can connect the veteran’s diagnosis to the specific toxic exposure event.
Medical Literature: Peer-reviewed research and scientific studies may support the relationship between certain exposures and medical conditions.
Treatment Records: Long-term treatment records can help establish frequency and severity.
Exposure Documentation: Additional records may help clarify the extent, duration, and nature of toxic exposures.
When a Nexus Letter May Help
A nexus letter can be particularly valuable when:
The condition isn’t presumptive
A VA exam resulted in a negative opinion
Medical literature supports a relationship
The exposure history is well documented
Multiple risk factors exist and require clarification
>> PRO TIP: The strongest nexus letters explain not only why the condition is related to your service, but also why alternative causes are less likely.
Conclusion
A TERA concession is an important favorable finding, but it is not the same as establishing service connection.
You’ll still need a current diagnosis and a medical nexus linking your condition to your military service.
If your claim was denied despite a conceded TERA, the missing piece is often medical evidence connecting the exposure to the diagnosed condition.
Understanding the difference between exposure and causation can help you identify weaknesses in your claim and build a stronger case moving forward.
FAQs | Frequently Asked Questions
Does a TERA concession mean my VA claim will be approved?
No. A TERA concession only confirms that a qualifying toxic exposure occurred during military service. The VA still requires evidence of a current disability and a nexus connecting the condition to that exposure.
Can the VA deny my claim even if toxic exposure is conceded?
Yes. Many claims are denied because the VA determines the medical evidence doesn’t establish a connection between the exposure and the diagnosed condition.
What is the difference between a TERA concession and service connection?
A TERA concession acknowledges exposure. Service connection requires evidence showing that the exposure caused or contributed to a current disability.
What conditions qualify under TERA?
TERA can apply to a wide range of toxic exposures. For non-presumptive conditions, a TERA concession may help establish in-service exposure, but veterans typically still need evidence linking their condition to that exposure.
What if my C&P examiner gave a negative opinion?
You may be able to challenge the opinion by submitting additional medical evidence, a nexus letter, or an independent medical opinion that addresses the examiner’s conclusions.
Do I need a nexus letter for a TERA claim?
Not always. However, a nexus letter can be helpful when the condition is not presumptive or when the VA has issued a negative medical opinion.
Can I appeal a TERA-related denial?
Yes. Veterans may pursue options such as a Supplemental Claim, Higher-Level Review, or Board Appeal depending on the circumstances of the denial.
What We Believe
Our WHY
We believe millions of veterans feel overlooked, lowballed, denied, or lost in the VA claims process.
Our purpose is to help underrated disabled veterans rated 0% to 90% create real life change by pursuing the VA disability benefits they legally, morally, ethically, and medically deserve.
We are INSIDERS.
Our HOW
We make the VA disability process easier through expert-level education, proven resources, and veteran-to-veteran support.
You are never alone in this fight.
Our flagship program, VA Claims Insider Elite, connects each veteran with an expert-level Veteran Coach who guides them through our proprietary 8-step process.
That process is built around our SEM Method:
Strategy + Education + Medical Evidence = VA Rating You Deserve!
Our WHAT
We help underrated disabled veterans rated 0% to 90% win, service connect, and increase their VA rating through a smarter strategy, better education, and stronger medical evidence.
YOU SERVED. YOU DESERVE.
Do you have the VA rating you were given…or the VA rating you actually deserve?
Because getting a decision from the VA does not always mean you got the right decision from the VA.
If you are rated anywhere from 0% to 90% and feel stuck, frustrated, underrated, denied, or overlooked, I am speaking directly to you.
And if you have never filed because you thought other veterans deserved it more, because you got denied before, or because you assumed it was too late, do not let those myths make your decision for you.
At VA Claims Insider, we help underrated disabled veterans create real life change by getting the VA rating and compensation they deserve!
Here’s a sliver of what you get when you join us:
A Veteran Coach by your side, so you never have to fight the VA alone.
A smarter, personalized strategy for your claim.
Better VA disability education, so you know what to do next.
Stronger private medical evidence (DBQs, Nexus Letters, Mental Health Evaluations, and more) at members-only rates to support the rating you deserve.
And a proven battle plan toward VA claim victory.
But maybe you’re wondering: Will this actually work for me?
That is a fair question.
At VA Claims Insider, we have helped 50,000+ veterans fight for the VA disability benefits they earned.
Our internal data shows an average *33% VA rating increase for veterans who complete our Elite program.
Our internal data also shows veterans in our programs get their claims approved *25% faster on average than the VA’s published average claim-processing timelines.
Veterans in our community have left 7,000+ total reviews, with a 4.6 out of 5 average rating.
More than 5,500 reviews are 5 stars, and 92% of all veteran customer reviews are either 4 or 5 stars.
*Based on VA Claims Insider internal data for veterans who completed the Elite program. Average results shown; individual results vary. No guaranteed outcome or faster claim processing.
If you are ready for a better battle plan, a smarter strategy, and the right path to the VA rating and compensation you deserve, we’ve got your six.
Call us now at 737-295-2226 or click the red button below to get started:
Katie McCarthy is a writer and editor with experience in daily news and digital and print magazine publishing. She honed her editorial (and firearms) skills at Guns & Ammo before helping launch Black Rifle Coffee Company’s Coffee or Die Magazine as the managing editor. She holds degrees in English (BA) and public administration (MPA). Katie is a military spouse and word nerd who enjoys reading, hiking, camping, gardening, and spending time with her family.
Understanding the difference between a 30% and 50% VA rating for migraines can affect both your monthly compensation and the strength of your claim.
While both VA ratings involve severe migraine attacks, the 50% rating usually requires evidence showing migraines are more frequent, more debilitating, and significantly interfere with your ability to work.
This guide breaks down the key differences between a 30% and 50% migraine rating, the evidence the VA looks for, and what may support a VA disability increase.
Summary of Key Points
A 50% migraine VA rating usually requires very frequent, completely prostrating attacks that significantly interfere with work.
You can still work and qualify for a 50% migraine rating if migraines cause severe economic impairment.
Strong migraine logs, medical records, and work-related evidence can play a significant role in supporting a higher rating.
Table of Contents
How the VA Rates Migraines
The VA rates migraines under diagnostic code (DC) 8100 at 0%, 10%, 30%, or 50%.
Ratings depend on the frequency, severity, and duration of prostrating attacks, along with how much the condition affects your ability to work and function in daily life.
When it comes to a 30% or 50% rating, the biggest difference is usually how often migraines occur and how severely they interfere with your ability to work.
Here’s a side-by-side breakdown of the key differences between a 30% and 50% migraine VA rating.
VA Rating
VA Criteria
What it Often Looks Like
30% Migraine VA Rating
Migraines with characteristic prostrating attacks occurring on average once a month over the last several months
You need to lie down in a dark room, miss occasional work, or isolate until symptoms improve
50% Migraine VA Rating
Migraines with very frequent, completely prostrating and prolonged attacks, productive of severe economic inadaptability
Frequent absences, leaving work early, difficulty maintaining reliable employment, or ongoing disruption to daily functioning
Understanding “Severe Economic Inadaptability”
The phrase “severe economic inadaptability” is a key factor in the 50% VA rating for migraines and means your symptoms significantly interfere with your ability to work.
The VA doesn’t require you to be unemployed to qualify. However, your migraines generally need to cause substantial work-related impairment.
Examples may include:
Frequent absences from work
Reduced productivity
Leaving work early because of migraines
Difficulty maintaining reliable employment
Missed promotions or disciplinary issues tied to migraine symptoms
What Does “Completely Prostrating” Mean?
A 50% migraine VA rating requires “completely prostrating” attacks, which are more severe than standard prostrating migraines.
Completely prostrating migraines leave you unable to function during an attack. Symptoms may force you to stop all activity, lie down for extended periods, avoid light or noise, and isolate until symptoms improve.
This is one of the biggest differences between a 30% and 50% migraine VA rating.
How to Get a 50% Migraine VA Rating
While nothing is guaranteed, the strongest migraine claims usually include evidence clearly documenting the frequency, severity, and duration of attacks.
Employer records showing missed work or accommodations
Documentation of time spent lying down during attacks
Your migraine C&P exam is also important, as the examiner’s findings often play a significant role in how the VA evaluates the severity of your migraines and assigns a rating.
Why Veterans Get Stuck at 30%
Many veterans experience migraines severe enough to qualify for a 50% VA rating but struggle to prove the level of work impairment required by the VA.
Occasionally, medical records confirm migraines but fail to clearly document how often attacks occur, how long they last, or how significantly they interfere with employment and daily functioning.
Without detailed evidence showing severe economic impairment, the VA may continue with a 30% migraine rating even when symptoms are much more disabling.
Can You Increase a 30% Migraine VA Rating to 50%?
Yes! A 30% migraine rating doesn’t prevent you from qualifying for a higher evaluation later.
If your migraines become more frequent, more severe, longer lasting, or more disruptive to your ability to work, you may qualify for a 50% migraine VA rating.
To increase your VA rating for migraines, your evidence should clearly show very frequent completely prostrating attacks and significant work impairment.
Think Your Migraine VA Rating Is Too Low?
Some veterans with severe migraines remain stuck at 30% because the evidence in their file fails to fully show how often attacks occur.
The difference between a 30% and 50% migraine rating often comes down to the quality of your evidence and how clearly your records document severe economic impairment.
At VA Claims Insider, our team works with veterans to build stronger, more complete claims backed by detailed medical and lay evidence.
What’s the difference between a 30% and 50% migraine VA rating?
The biggest difference is the frequency and severity of attacks, along with how much migraines interfere with your ability to work. A 50% migraine VA rating usually requires very frequent, completely prostrating attacks that cause severe economic impairment.
How often do migraines need to occur for a 50% VA rating?
The VA doesn’t give an exact number of migraines required for a 50% rating. However, attacks usually need to be very frequent and severe enough to significantly interfere with your ability to work.
How can you increase a 30% migraine VA rating to 50%?
You may qualify for a 50% migraine VA rating if your evidence shows migraines are more frequent, more severe, longer lasting, or more disruptive to your ability to work. Helpful evidence may include migraine logs, a current and credible DBQ showing symptoms and impact, medical records, missed work documentation, and lay statements.
Can migraines be secondary to another VA disability?
Yes. Migraines are commonly linked to conditions like PTSD, tinnitus, TBI, anxiety, depression, and sleep apnea.
Can you work with a 50% migraine VA rating?
Yes. You can still work and qualify for a 50% migraine VA rating if your migraines cause severe economic impairment, such as frequent absences or reduced productivity.
Do migraine logs help a VA claim?
Yes. Migraine logs can strengthen a claim by documenting the frequency, duration, severity, and work impact of attacks over time.
What We Believe
Our WHY
We believe millions of veterans feel overlooked, lowballed, denied, or lost in the VA claims process.
Our purpose is to help underrated disabled veterans rated 0% to 90% create real life change by pursuing the VA disability benefits they legally, morally, ethically, and medically deserve.
We are INSIDERS.
Our HOW
We make the VA disability process easier through expert-level education, proven resources, and veteran-to-veteran support.
You are never alone in this fight.
Our flagship program, VA Claims Insider Elite, connects each veteran with an expert-level Veteran Coach who guides them through our proprietary 8-step process.
That process is built around our SEM Method:
Strategy + Education + Medical Evidence = VA Rating You Deserve!
Our WHAT
We help underrated disabled veterans rated 0% to 90% win, service connect, and increase their VA rating through a smarter strategy, better education, and stronger medical evidence.
YOU SERVED. YOU DESERVE.
Do you have the VA rating you were given…or the VA rating you actually deserve?
Because getting a decision from the VA does not always mean you got the right decision from the VA.
If you are rated anywhere from 0% to 90% and feel stuck, frustrated, underrated, denied, or overlooked, I am speaking directly to you.
And if you have never filed because you thought other veterans deserved it more, because you got denied before, or because you assumed it was too late, do not let those myths make your decision for you.
At VA Claims Insider, we help underrated disabled veterans create real life change by getting the VA rating and compensation they deserve!
Here’s a sliver of what you get when you join us:
A Veteran Coach by your side, so you never have to fight the VA alone.
A smarter, personalized strategy for your claim.
Better VA disability education, so you know what to do next.
Stronger private medical evidence (DBQs, Nexus Letters, Mental Health Evaluations, and more) at members-only rates to support the rating you deserve.
And a proven battle plan toward VA claim victory.
But maybe you’re wondering: Will this actually work for me?
That is a fair question.
At VA Claims Insider, we have helped 50,000+ veterans fight for the VA disability benefits they earned.
Our internal data shows an average *33% VA rating increase for veterans who complete our Elite program.
Our internal data also shows veterans in our programs get their claims approved *25% faster on average than the VA’s published average claim-processing timelines.
Veterans in our community have left 7,000+ total reviews, with a 4.6 out of 5 average rating.
More than 5,500 reviews are 5 stars, and 92% of all veteran customer reviews are either 4 or 5 stars.
*Based on VA Claims Insider internal data for veterans who completed the Elite program. Average results shown; individual results vary. No guaranteed outcome or faster claim processing.
If you are ready for a better battle plan, a smarter strategy, and the right path to the VA rating and compensation you deserve, we’ve got your six.
Call us now at 737-295-2226 or click the red button below to get started:
Kelly Olone is a military spouse who earned her degree in Psychology from Florida International University. After working in the non-profit sector for several years, she turned to her passion for writing. She aims to contribute to a better understanding of the valuable benefits that veterans deserve. As a mom, Kelly navigates the delicate balance between deadlines and bedtime stories with finesse.
In this ultimate guide, VA disability expert and bestselling author Brian Reese reveals and explains the 100 most common VA disability claims.
While there are over 1,000 conditions eligible for VA disability benefits, these 100 conditions are among the most commonly claimed and service-connected disabilities for veterans.
Methodology: The updated top 10 list comes from the newly released VBA’s 2025 disability compensation data. The next 40 come from the Top 50 VA Disability Claims list, and the remaining 50 come from our Top 100 Most Common VA Disability Claims guide and rating criteria.
Let’s begin!
Table of Contents
Top 100 Most Common VA Disability Claims
1. Tinnitus
Tinnitus is the perception of sound, such as ringing, buzzing, humming, roaring, or clicking, without an external sound source. For veterans, tinnitus is commonly associated with military noise exposure from weapons, aircraft, explosions, engines, generators, heavy equipment, flight lines, shipboard noise, and combat environments.
VA rates recurrent tinnitus under 38 CFR Part 4, Diagnostic Code 6260, at 10%. There is no higher schedular rating for tinnitus, and VA assigns only one 10% rating whether the tinnitus is perceived in one ear, both ears, or in the head. The strongest evidence usually includes a current diagnosis, credible noise exposure history, and a clear statement explaining when the ringing began and how it has continued since service.
2. Limitation of Flexion of the Knee
Limitation of flexion of the knee means the veteran cannot bend the knee normally due to pain, stiffness, arthritis, ligament injury, meniscus problems, cartilage damage, overuse, or trauma. This is one of the most common musculoskeletal VA claims because military service is hard on the knees from running, rucking, jumping, kneeling, climbing, and repetitive impact.
VA rates limitation of flexion of the knee under DC 5260 at 0%, 10%, 20%, or 30%. Flexion limited to 60 degrees is 0%, 45 degrees is 10%, 30 degrees is 20%, and 15 degrees is 30%. Veterans should make sure the exam captures painful motion, flare-ups, repeated-use limitations, instability, swelling, difficulty with stairs, and how the knee condition affects work and daily life.
3. Paralysis of the Sciatic Nerve (Sciatica)
Sciatica is pain, numbness, tingling, burning, or weakness that travels along the sciatic nerve, often from the low back into the buttock, hip, leg, calf, or foot. It is commonly secondary to lumbosacral strain, degenerative disc disease, spinal stenosis, herniated discs, or other lumbar spine conditions.
VA rates sciatic nerve paralysis under DC 8520 at 10%, 20%, 40%, 60%, or 80%. The rating depends on whether the impairment is mild, moderate, moderately severe, severe with marked muscular atrophy, or complete paralysis. If both legs are affected, VA can rate the right and left lower extremities separately, so the evidence should clearly document symptoms in each leg.
4. Lumbosacral or Cervical Strain
Lumbosacral strain affects the low back, while cervical strain affects the neck. These conditions are extremely common in veterans due to lifting, carrying heavy gear, airborne operations, vehicle accidents, physical training, prolonged sitting in tactical vehicles, and years of military wear and tear.
VA rates lumbosacral or cervical strain under DC 5237 using the General Rating Formula for Diseases and Injuries of the Spine. Ratings can be 10%, 20%, 30%, 40%, 50%, or 100%, depending on range of motion, ankylosis, muscle spasm, guarding, abnormal gait, abnormal spinal contour, and functional loss. Associated neurological abnormalities, such as radiculopathy, sciatica, bowel impairment, or bladder impairment, may be rated separately when supported by the evidence.
5. Post Traumatic Stress Disorder (PTSD)
PTSD is a mental health condition that can develop after trauma, combat, military sexual trauma, serious accidents, fear of hostile military or terrorist activity, or exposure to death, injury, or threatened harm. PTSD can affect sleep, relationships, mood, anger, work performance, concentration, judgment, and the ability to function around other people.
VA rates PTSD under DC 9411 using the General Rating Formula for Mental Disorders at 0%, 10%, 30%, 50%, 70%, or 100%. VA evaluates the level of occupational and social impairment, along with the frequency, severity, duration, and functional impact of symptoms. Strong PTSD claims document the stressor, diagnosis, treatment, symptoms, and real-world impairment at work, home, and socially.
6. Hearing Loss
Hearing loss is reduced ability to hear speech, sounds, or certain frequencies. Veterans commonly develop hearing loss from acoustic trauma, including weapons fire, aircraft, machinery, explosions, engines, shipboard noise, and other hazardous military noise exposure.
VA rates hearing loss under DC 6100 from 0% to 100% using a mechanical formula based on puretone threshold averages and Maryland CNC speech discrimination testing performed by a state-licensed audiologist. Many veterans are service connected for hearing loss at 0%, which still matters because it establishes service connection and allows the veteran to file for an increase if hearing worsens later.
7. Limitation of Motion of the Arm
Limitation of motion of the arm most often involves the shoulder, although different diagnostic codes apply to the elbow, wrist, hand, and fingers. Shoulder limitation is common in veterans due to rotator cuff injuries, dislocations, arthritis, labral tears, repetitive lifting, push-ups, pull-ups, overhead work, and trauma.
VA commonly rates shoulder limitation of motion under DC 5201. Ratings generally range from 20% to 40% for the major arm and 20% to 30% for the minor arm, depending on whether flexion or abduction is limited to shoulder level, midway between the side and shoulder level, or 25 degrees from the side. The evidence should document painful motion, weakness, flare-ups, repeated-use loss, and limitations with lifting, reaching, dressing, and overhead activity.
8. Scars, Burns (2nd Degree)
Burn scars can result from thermal burns, chemical burns, explosions, electrical injuries, fires, surgeries, or traumatic injuries during service. VA evaluates scars based on location, size, pain, instability, tissue damage, disfigurement, and whether the scar causes limitation of function.
VA rates burn scars under the applicable scar codes, including DC 7800, 7801, 7802, 7804, and 7805. Ratings can range from 0% to 80%, depending on whether the scar affects the head, face, or neck, is deep or associated with underlying soft tissue damage, covers a large area, is painful or unstable, or causes functional impairment. Painful or unstable scars under DC 7804 can be rated 10%, 20%, or 30%, depending on the number of qualifying scars.
9. Migraines (Headaches)
Migraines are a neurological condition involving recurrent headaches that can become severe enough to force a veteran to lie down, stop working, avoid light or sound, or miss daily activities. Migraines can be claimed directly, secondarily, or as residuals of TBI, tinnitus, neck conditions, sleep problems, mental health conditions, or medication side effects.
VA rates migraines under DC 8100 at 0%, 10%, 30%, or 50%. The rating depends on characteristic prostrating attacks, frequency, duration, and whether the migraines are productive of severe economic inadaptability. A migraine log is powerful evidence because it can document frequency, severity, duration, medication use, missed work, reduced productivity, and whether the veteran had to lie down in a dark or quiet room.
10. Limitation of Motion of the Ankle
Limitation of motion of the ankle means the ankle cannot move normally because of pain, stiffness, arthritis, sprain residuals, fracture residuals, tendon problems, instability, or other injury. Ankle claims are common because military service involves running, marching, jumping, uneven terrain, boots, load carriage, and repetitive stress.
VA rates limitation of motion of the ankle under DC 5271 at 10% for moderate limitation and 20% for marked limitation. Current criteria define moderate limitation as less than 15 degrees dorsiflexion or less than 30 degrees plantar flexion, and marked limitation as less than 5 degrees dorsiflexion or less than 10 degrees plantar flexion. Ankle ankylosis under DC 5270 can rate 20%, 30%, or 40%, depending on position and severity.
11. Degenerative Arthritis of the Spine
Degenerative arthritis of the spine is wear-and-tear arthritis affecting the cervical, thoracic, or lumbar spine. It can cause pain, stiffness, muscle spasm, limited motion, abnormal gait, and nerve symptoms when arthritis contributes to foraminal narrowing or nerve irritation.
VA usually rates degenerative arthritis of the spine under DC 5242 using the General Rating Formula for the Spine, with possible ratings of 10%, 20%, 30%, 40%, 50%, or 100%. If the spine condition causes neurological symptoms, such as radiculopathy, sciatica, bowel impairment, or bladder impairment, those residuals may be evaluated separately. The key evidence is range of motion, pain, flare-ups, abnormal gait, and any separately diagnosable nerve involvement.
12. Sleep Apnea
Sleep apnea is a sleep-related breathing disorder where breathing repeatedly stops, decreases, or becomes obstructed during sleep. Veterans often claim sleep apnea directly or secondarily to allergic rhinitis, sinusitis, asthma, PTSD, weight gain caused by service-connected conditions, medications, or other disabilities.
VA rates sleep apnea under DC 6847 at 0%, 30%, 50%, or 100%. A 0% rating applies when sleep apnea is documented but asymptomatic; 30% is for persistent daytime hypersomnolence; 50% is for required use of a breathing assistance device such as a CPAP; and 100% is for chronic respiratory failure with carbon dioxide retention or cor pulmonale, or when a tracheostomy is required. The sleep study proves the diagnosis, but the nexus usually wins the claim.
13. Traumatic Brain Injury (TBI)
A traumatic brain injury is caused by a blow, blast, fall, vehicle accident, explosion, impact, or other trauma to the head. TBI residuals may include cognitive problems, headaches, dizziness, balance problems, irritability, sleep issues, memory problems, light sensitivity, sound sensitivity, and neurological symptoms.
VA rates TBI under DC 8045 using the table for cognitive impairment and other residuals, with overall evaluations that can result in 0%, 10%, 40%, 70%, or 100%. Separate ratings may apply for distinct diagnoses such as migraines, seizures, vertigo, hearing loss, tinnitus, neurogenic bladder, smell or taste loss, or a diagnosed mental health condition, but VA cannot rate the same symptom twice. Strong TBI claims identify each residual clearly and avoid pyramiding.
14. Major Depressive Disorder
Major depressive disorder is a mental health condition involving persistent depressed mood, loss of interest, low motivation, sleep impairment, fatigue, poor concentration, irritability, appetite changes, feelings of worthlessness, and social withdrawal. It can be directly related to service or secondary to chronic pain, tinnitus, cancer, medical conditions, or other service-connected disabilities.
VA rates major depressive disorder under DC 9434 using the General Rating Formula for Mental Disorders at 0%, 10%, 30%, 50%, 70%, or 100%. VA evaluates occupational and social impairment, including how symptoms affect work, relationships, judgment, mood, reliability, productivity, and daily functioning. The diagnosis matters, but the rating is driven by severity and functional impairment.
15. Asthma
Asthma is a chronic respiratory condition involving airway inflammation and narrowing, which can make breathing difficult. Veterans may develop asthma or worsening asthma due to burn pits, dust, smoke, chemicals, environmental exposures, respiratory infections, exercise, or other service-related triggers.
VA rates bronchial asthma under DC 6602 at 10%, 30%, 60%, or 100%. Ratings are based on pulmonary function tests, use of inhalational or oral bronchodilator therapy, inhalational anti-inflammatory medication, systemic corticosteroid use, physician visits for exacerbations, attacks with respiratory failure, and immunosuppressive medication. Medication records, pulmonary function testing, ER visits, and pulmonology notes can strongly support the rating.
16. Diabetes Type 2
Diabetes Type 2 is a chronic metabolic condition where the body has difficulty regulating blood sugar. It is commonly associated with Agent Orange exposure and can also produce secondary complications involving the nerves, kidneys, eyes, heart, feet, skin, and reproductive system.
VA rates diabetes mellitus under DC 7913 at 10%, 20%, 40%, 60%, or 100%. A 10% rating generally involves restricted diet; 20% involves insulin and restricted diet or oral hypoglycemic medication and restricted diet; 40% adds regulation of activities; and higher ratings involve more severe treatment, hospitalizations, frequent diabetic care, weight or strength loss, and complications. Complications such as peripheral neuropathy, kidney disease, eye disease, and erectile dysfunction may be separately rated if compensable.
17. Cancer
Cancer refers to malignant growths in the body, and VA ratings depend on the specific cancer, body system affected, whether the cancer is active, whether treatment is ongoing, and what residuals remain after treatment. Many veterans claim cancer based on toxic exposure, radiation exposure, Agent Orange exposure, burn pit exposure, or other service-related risk factors.
VA typically rates active malignant neoplasms at 100% under the body-system code for the specific cancer during active disease or treatment. After treatment ends, VA usually schedules a mandatory review and then rates residuals if there is no recurrence or metastasis. Residuals can include fatigue, neuropathy, organ damage, urinary issues, bowel problems, scars, endocrine problems, sexual dysfunction, and mental health symptoms.
18. Generalized Anxiety Disorder
Generalized anxiety disorder involves excessive worry, fear, tension, restlessness, irritability, poor concentration, muscle tension, panic symptoms, avoidance, and sleep impairment. It can be directly related to military service or secondary to tinnitus, chronic pain, PTSD, medical conditions, medications, or other service-connected disabilities.
VA rates generalized anxiety disorder under DC 9400 using the General Rating Formula for Mental Disorders at 0%, 10%, 30%, 50%, 70%, or 100%. VA evaluates the frequency, severity, duration, and functional impact of symptoms, along with occupational and social impairment. Veterans should describe how anxiety affects work, relationships, sleep, decision-making, reliability, and ability to function around others.
19. Pes Planus (Flat Feet)
Pes planus, commonly called flat feet, occurs when the arches of the feet collapse or flatten. It can be caused or aggravated by military boots, marching, running, prolonged standing, carrying heavy loads, or service aggravation of preexisting flat feet.
VA rates pes planus under DC 5276 at 0%, 10%, 20%, 30%, or 50%. Mild symptoms relieved by arch supports are 0%; moderate unilateral or bilateral flat feet can rate 10%; severe unilateral can rate 20%; severe bilateral can rate 30%; pronounced unilateral can rate 30%; and pronounced bilateral can rate 50%. Key evidence includes pain on use, swelling, callosities, deformity, pronation, Achilles tendon alignment, and whether orthotics help.
20. Radiculopathy
Radiculopathy occurs when a nerve root is compressed, irritated, or damaged, often due to a cervical or lumbar spine condition. It can cause radiating pain, numbness, tingling, burning, weakness, reduced reflexes, and symptoms traveling from the spine into an arm or leg.
VA rates radiculopathy under the affected nerve or radicular group. Lower extremity radiculopathy is often rated under the sciatic nerve at 10%, 20%, 40%, 60%, or 80%, or under the femoral nerve at 10%, 20%, 30%, or 40%, depending on severity. Upper extremity radiculopathy may be rated under radicular group or specific nerve codes. The evidence should identify the affected nerve, side, severity, sensory loss, motor loss, reflex changes, and functional impact.
21. Adjustment Disorder
Adjustment disorder is a mental health condition that occurs when a person has difficulty coping with a stressful life event, trauma, transition, injury, medical condition, or major change. Veterans may develop adjustment disorder due to military stress, deployments, transition out of service, chronic pain, family stress, injury, or service-connected health problems.
VA rates adjustment disorder under DC 9440 using the General Rating Formula for Mental Disorders at 0%, 10%, 30%, 50%, 70%, or 100%. The diagnosis alone does not determine the rating; occupational and social impairment does. Evidence should document mood symptoms, anxiety, sleep problems, anger, motivation issues, concentration problems, relationship strain, and impact on work and daily functioning.
Somatic symptom disorder involves distress, anxiety, or impairment related to physical symptoms such as chronic pain, fatigue, dizziness, or other persistent symptoms. Veterans may develop this condition when service-connected physical conditions create ongoing pain, fear, functional loss, and emotional distress.
VA rates somatic symptom disorder under DC 9421 using the General Rating Formula for Mental Disorders at 0%, 10%, 30%, 50%, 70%, or 100%. VA generally evaluates mental health symptoms together when they overlap, so the key is to ensure all symptoms and functional impairment are captured in the overall mental health evaluation. Evidence should connect the symptoms to service or to a service-connected condition and document how they affect work and daily life.
23. Gastroesophageal Reflux Disease (GERD)
GERD is a digestive condition where stomach acid or contents flow back into the esophagus, causing reflux, heartburn, regurgitation, chest discomfort, coughing, hoarseness, nausea, and swallowing problems. It can be linked to medications, NSAID use, weight gain, hiatal hernia, mental health conditions, or other service-connected disabilities.
Under current VA rules, GERD is rated under DC 7206 at 0%, 10%, 30%, 50%, or 80%. The rating criteria focus heavily on documented esophageal stricture history, dysphagia, daily medication, dilation, steroid dilation, stent placement, aspiration, undernutrition, substantial weight loss, PEG tube, or surgical correction. Evidence such as endoscopy, barium swallow, CT, medication history, and documented swallowing problems is especially important.
24. Irritable Bowel Syndrome (IBS)
IBS is a functional gastrointestinal disorder involving abdominal pain related to bowel movements and changes in bowel habits. It is common among Gulf War veterans and may also be linked to stress, mental health conditions, medications, or other service-connected disabilities.
VA rates IBS under DC 7319 at 10%, 20%, or 30%, with a 0% possible when compensable criteria are not met. Ratings are based on abdominal pain related to defecation and bowel symptoms such as changed stool frequency, changed stool form, urgency, straining, mucus, bloating, or distension. A bowel symptom log can help document frequency, urgency, accidents, pain, and impact on work or daily life.
25. Erectile Dysfunction
Erectile dysfunction is the inability to achieve or maintain an erection sufficient for sexual activity. It is commonly secondary to diabetes, hypertension, heart disease, prostate conditions, PTSD, depression, anxiety, medications, back injuries, nerve conditions, or other service-connected disabilities.
Under current VA rules, erectile dysfunction with or without penile deformity is rated under DC 7522 at 0% schedularly. However, VA should consider Special Monthly Compensation for loss of use of a creative organ when supported by the evidence. The key is documenting the diagnosis, cause or aggravation, medication history, and relationship to service or a service-connected disability.
26. Plantar Fasciitis
Plantar fasciitis is inflammation or degeneration of the plantar fascia, the thick band of tissue along the bottom of the foot. Veterans often develop plantar fasciitis from running, rucking, marching, boots, prolonged standing, hard surfaces, and repetitive military training.
VA rates plantar fasciitis under DC 5269 at 10%, 20%, 30%, or 40%. A 10% rating applies otherwise; 20% applies when unilateral plantar fasciitis has no relief from both non-surgical and surgical treatment; 30% applies when bilateral plantar fasciitis has no relief from both non-surgical and surgical treatment; and 40% applies with actual loss of use of the foot. Evidence should document heel pain, arch pain, orthotics, injections, physical therapy, surgery, and whether treatment helped.
27. Arthritis
Arthritis is joint inflammation, degeneration, or damage that can cause pain, stiffness, swelling, weakness, and reduced motion. Veterans commonly develop arthritis from injuries, overuse, airborne operations, physical training, repetitive stress, trauma, and service aggravation.
Degenerative arthritis is usually rated under DC 5003 or the specific joint’s limitation-of-motion diagnostic code. Ratings vary by joint, but DC 5003 can support 10% or 20% in certain x-ray-confirmed multi-joint cases when limitation of motion is otherwise noncompensable. Painful motion, flare-ups, x-ray evidence, functional loss, and repeated-use limitations should be documented.
28. Hypertension (High Blood Pressure)
Hypertension is chronically elevated blood pressure. It can be claimed directly, presumptively in certain exposure situations, or secondarily to kidney disease, sleep apnea, PTSD, medication effects, endocrine conditions, or other service-connected disabilities.
VA rates hypertension under DC 7101 at 10%, 20%, 40%, or 60%. Ratings depend on predominant systolic and diastolic readings and whether there is a history of diastolic pressure predominantly 100 or more requiring continuous medication. VA generally requires blood pressure readings taken two or more times on at least three different days, so multiple readings over time are critical.
29. Degenerative Disc Disease (DDD)
Degenerative disc disease is a spine condition where spinal discs lose height, bulge, herniate, or degenerate, often causing back or neck pain and sometimes nerve compression. DDD is common in veterans due to years of military wear and tear, lifting, impact, vehicle vibration, trauma, and repetitive load-bearing.
VA usually rates DDD under DC 5242 using the General Rating Formula for the Spine unless intervertebral disc syndrome applies under DC 5243. Spine ratings can range from 10% to 100%, while IVDS can be rated at 10%, 20%, 40%, or 60% based on physician-prescribed bed rest for incapacitating episodes. Separate ratings may apply for radiculopathy or other neurological abnormalities.
30. Carpal Tunnel Syndrome (CTS)
Carpal tunnel syndrome occurs when the median nerve is compressed at the wrist. Veterans may develop CTS from repetitive gripping, typing, maintenance work, mechanical work, weapons handling, vibration tools, or other repetitive hand and wrist activities.
VA usually rates carpal tunnel syndrome under median nerve impairment, DC 8515. Ratings can range from 10% to 70%, depending on mild, moderate, severe, or complete paralysis and whether the major or minor hand is affected. Evidence should document numbness, tingling, weakness, dropping objects, grip problems, EMG or nerve conduction findings, and functional limitations.
31. Chronic Fatigue Syndrome (CFS)
Chronic fatigue syndrome is a complex condition involving persistent, debilitating fatigue that is not substantially relieved by rest and is not fully explained by another condition. It is commonly associated with Gulf War service and may involve cognitive impairment, post-exertional worsening, headaches, sleep disturbance, and widespread pain.
VA rates CFS under DC 6354 at 10%, 20%, 40%, 60%, or 100%. Ratings are based on debilitating fatigue, cognitive impairment, restriction of routine daily activities compared to pre-illness levels, medication control, and periods of incapacitation. Strong evidence should show how fatigue limits daily life, work, exercise, concentration, and routine activities.
32. Fibromyalgia
Fibromyalgia is a chronic condition involving widespread musculoskeletal pain and tender points, often with fatigue, sleep disturbance, stiffness, headaches, IBS symptoms, depression, anxiety, and cognitive problems. It is a common Gulf War-related claim and can significantly affect daily function.
VA rates fibromyalgia under DC 5025 at 10%, 20%, or 40%. Ratings depend on widespread pain and tender points, associated symptoms, whether continuous medication is required, frequency of exacerbations, and whether symptoms are constant or nearly constant and refractory to therapy. The maximum schedular rating for fibromyalgia is 40%, but distinct secondary or separate conditions may also matter if not duplicative.
33. Eczema
Eczema is a chronic inflammatory skin condition that can cause itchy, red, dry, cracked, scaly, or inflamed skin. Veterans may develop eczema from environmental exposures, chemicals, uniforms, stress, heat, sweat, deployment conditions, or allergic triggers.
VA rates eczema under DC 7806 using the General Rating Formula for the Skin at 0%, 10%, 30%, or 60%. Ratings are based on the percentage of the entire body or exposed areas affected and the type and duration of therapy, including topical or systemic treatment. Photos during flare-ups, dermatology records, prescription history, and evidence of systemic therapy are important.
34. Allergic Rhinitis (Hay Fever)
Allergic rhinitis is inflammation of the nasal passages caused by allergens or irritants. Veterans may develop or aggravate rhinitis from dust, burn pits, smoke, chemicals, sand, pollen, environmental hazards, or other service-related exposures.
VA rates allergic rhinitis under DC 6522 at 10% or 30%, with a 0% possible when compensable criteria are not met. A 10% rating applies without polyps but with greater than 50% obstruction of both nasal passages or complete obstruction on one side, and 30% applies with polyps. ENT records, nasal exams, imaging, and documentation of obstruction or polyps can make the difference.
35. Sinusitis
Sinusitis is inflammation or infection of the sinuses and may be acute, recurrent, or chronic. It is common among veterans exposed to burn pits, dust, sand, smoke, chemicals, fumes, and other airborne hazards.
VA rates sinusitis under DC 6510 through DC 6514 at 0%, 10%, 30%, or 50%. Ratings depend on incapacitating episodes requiring prolonged antibiotic treatment, non-incapacitating episodes with headaches, pain, purulent discharge or crusting, surgery, osteomyelitis, and near-constant symptoms. Veterans should document infections, antibiotic use, headaches, pain, discharge, imaging, and surgeries.
36. Meniere’s Syndrome
Meniere’s syndrome is an inner ear disorder that can cause episodes of vertigo, hearing impairment, tinnitus, ear fullness, imbalance, nausea, vomiting, and falls. It can be highly disabling when attacks are frequent or unpredictable.
VA rates Meniere’s syndrome under DC 6205 at 30%, 60%, or 100%. Ratings are based on hearing impairment, vertigo attacks, tinnitus, and cerebellar gait. VA may alternatively rate hearing loss, tinnitus, and vertigo separately if that produces a higher combined evaluation, but VA cannot combine separate ratings with a rating under DC 6205 for the same symptoms.
Arteriosclerotic heart disease, also known as coronary artery disease, occurs when plaque builds up in the arteries that supply blood to the heart. Veterans may claim it directly, presumptively, or secondarily depending on exposure history, medical history, and service-connected conditions.
VA rates arteriosclerotic heart disease under DC 7005 using the General Rating Formula for Diseases of the Heart at 10%, 30%, 60%, or 100%. Ratings are based on METs workload, symptoms such as breathlessness, fatigue, angina, dizziness, syncope, heart failure, cardiac hypertrophy or dilatation, and medication. Cardiology records, stress tests, echocardiograms, METs estimates, and medication lists are key evidence.
38. Chronic Conjunctivitis
Chronic conjunctivitis is long-term inflammation of the conjunctiva, the tissue covering the white part of the eye and inner eyelids. It can be caused by infection, allergies, chemical exposure, irritants, environmental conditions, or eye trauma.
VA rates chronic nontrachomatous conjunctivitis under DC 6018. Active chronic conjunctivitis is evaluated under the General Rating Formula for Diseases of the Eye with a minimum 10% rating, while inactive conjunctivitis is rated based on residuals such as visual impairment or disfigurement. Eye exams, optometry or ophthalmology records, treatment visits, and photos can support the claim.
39. Limited Motion of the Jaw (Temporomandibular Disorder)
Limited motion of the jaw often involves temporomandibular disorder, jaw trauma, bruxism, malocclusion, or residuals of dental or facial injury. It can interfere with chewing, speaking, yawning, eating, and sleeping.
VA rates limited motion of the temporomandibular articulation under DC 9905 at 10%, 20%, 30%, 40%, or 50%. Ratings are based on interincisal range, lateral excursion, and mechanically required dietary restrictions verified by a physician. Evidence should include jaw measurements, dental or oral surgery records, pain, clicking, locking, chewing difficulty, and medically verified diet restrictions.
40. Hiatal Hernia
A hiatal hernia occurs when part of the stomach pushes upward through the diaphragm into the chest area. It often produces symptoms that overlap with GERD, including reflux, regurgitation, heartburn, chest discomfort, nausea, coughing, and swallowing difficulty.
Under current VA rules, hiatal hernia and paraesophageal hernia under DC 7346 are rated as esophageal stricture under DC 7203. Ratings can be 0%, 10%, 30%, 50%, or 80%, depending on documented stricture history, dysphagia, medication, dilation, stent placement, aspiration, undernutrition, substantial weight loss, PEG tube, or surgical correction. Endoscopy, barium swallow, CT, and treatment records are especially important.
41. Hemorrhoids
Hemorrhoids are swollen veins in or around the rectum and anus. They can cause rectal pain, itching, bleeding, swelling, thrombosis, prolapse, irritation, and discomfort while sitting or during bowel movements.
VA rates hemorrhoids under DC 7336 at 10% or 20%, with a 0% possible when compensable criteria are not met. A 20% rating requires persistent bleeding with anemia or continuously prolapsed internal hemorrhoids with frequent thrombosis. Veterans should document bleeding, anemia, thrombosis, prolapse, flare-ups, treatment, procedures, and frequency of symptoms.
42. Varicose Veins
Varicose veins are enlarged, twisted veins, usually in the legs, caused by poor venous circulation. Veterans may develop or aggravate varicose veins from prolonged standing, heavy load carriage, trauma, vascular strain, or service-related activity.
VA rates varicose veins under DC 7120, using the criteria for post-phlebitic syndrome under DC 7121, at 0%, 10%, 20%, 40%, 60%, or 100% per affected extremity. Ratings are based on aching, fatigue, edema, relief with elevation or compression, stasis pigmentation, eczema, ulceration, subcutaneous induration, and constant pain at rest. Each leg can be evaluated separately when both are affected.
43. Nephrolithiasis (Kidney Stones)
Nephrolithiasis means kidney stones. Veterans with kidney stones may experience severe flank pain, blood in urine, painful urination, nausea, vomiting, urinary urgency, urinary frequency, infections, obstruction, and recurrent stone passage.
VA rates kidney stones under DC 7508, generally as hydronephrosis under DC 7509 unless recurrent stone formation supports a 30% rating. Ratings are typically 10%, 20%, or 30%, while severe cases may be rated as renal dysfunction up to 100%. Imaging, ER records, urology notes, procedures, recurrence history, diet therapy, and medication records are important evidence.
44. Hypothyroidism
Hypothyroidism occurs when the thyroid gland does not produce enough thyroid hormone. Symptoms may include fatigue, weight gain, cold intolerance, constipation, dry skin, depression, slowed heart rate, brain fog, muscle aches, and reduced energy.
VA rates hypothyroidism under DC 7903. Myxedema can be rated 100% until six months after stabilization of crisis, and hypothyroidism without myxedema is rated 30% for six months after initial diagnosis. After that period, VA rates residuals under the appropriate body system, such as cardiac, mental health, skin, endocrine, or other residual effects.
45. Anemia
Anemia is a blood condition involving reduced red blood cells, hemoglobin, or oxygen-carrying capacity. It can cause fatigue, weakness, dizziness, headaches, shortness of breath, pale skin, rapid heartbeat, cold hands or feet, and reduced exercise tolerance.
VA rates anemia based on the specific type, not one generic anemia code. Iron deficiency anemia under DC 7720 can be rated 0%, 10%, or 30%, depending on whether it is asymptomatic or controlled by diet, requires continuous oral supplementation, or requires IV iron infusions. Other anemia types may have different criteria, including higher or temporary ratings depending on severity and residuals.
46. Peripheral Neuropathy
Peripheral neuropathy is nerve damage affecting the extremities, often causing numbness, tingling, burning pain, electric shock sensations, weakness, balance problems, reduced sensation, and difficulty walking or gripping. It is commonly associated with diabetes, toxic exposure, chemotherapy, radiculopathy, and other neurological conditions.
VA rates peripheral neuropathy under the diagnostic code for the specific affected nerve. Ratings vary widely by nerve and severity; for example, sciatic nerve ratings can range from 10% to 80%, femoral nerve ratings from 10% to 40%, and median nerve ratings from 10% to 70%. The evidence should identify the nerve, side, severity, sensory loss, motor loss, reflex changes, atrophy, and functional impairment.
47. Prostate Gland Injuries
Prostate gland injuries and residuals can include prostatitis, prostate trauma, prostate surgery residuals, bladder outlet obstruction, or other prostate-related conditions. Common symptoms include urinary frequency, urgency, leakage, weak stream, nighttime urination, obstruction, infections, pelvic pain, and sexual dysfunction.
VA rates prostate gland injuries, infections, hypertrophy, postoperative residuals, and bladder outlet obstruction under DC 7527 as voiding dysfunction or urinary tract infection, whichever is predominant. Ratings depend on leakage, pad use, urinary frequency, nighttime voiding, obstruction, infections, and renal involvement. The strongest evidence usually documents urinary symptoms in detail.
48. Ischemic Heart Disease
Ischemic heart disease occurs when reduced blood flow to the heart causes chest pain, impaired cardiac function, heart attack, or other heart-related problems. It is one of the major presumptive conditions for certain exposed veterans and may also be claimed directly or secondarily.
VA commonly rates ischemic heart disease under DC 7005 using the General Rating Formula for Diseases of the Heart at 10%, 30%, 60%, or 100%. Ratings are based on METs, symptoms, medication, cardiac hypertrophy or dilatation, heart failure, and functional capacity. Veterans should submit cardiology records, stress testing, echocardiogram results, hospitalizations, stents, bypass history, and medication lists.
49. Vertigo
Vertigo is a sensation of spinning, dizziness, imbalance, or motion when no movement is occurring. It may be related to inner ear disorders, vestibular conditions, TBI, migraines, Meniere’s syndrome, tinnitus, or other service-connected conditions.
VA usually rates vertigo as a peripheral vestibular disorder under DC 6204 at 10% for occasional dizziness and 30% for dizziness with occasional staggering. Objective findings supporting vestibular disequilibrium are required. If Meniere’s syndrome applies, VA may rate under DC 6205 at 30%, 60%, or 100%, depending on the full disability picture.
50. Urinary Incontinence
Urinary incontinence is loss of bladder control. It can result from prostate conditions, neurological disease, spinal cord problems, TBI, diabetes, genitourinary surgery, or other service-connected conditions.
VA rates urinary incontinence as voiding dysfunction under 38 CFR § 4.115a at 20%, 40%, or 60%. Ratings are based on absorbent material use, how often absorbent materials must be changed, or whether an appliance is required. Veterans should document pad use per day, nighttime awakenings, leakage, urgency, accidents, appliance use, and daily impact.
51. Amputation Residuals
Amputation residuals are the ongoing effects after the loss or removal of a limb, finger, toe, hand, foot, or other body part. Residuals may include phantom limb pain, stump pain, prosthetic problems, balance issues, altered gait, weakness, skin breakdown, and difficulty with daily activities.
VA rates amputations under the specific diagnostic code for the affected body part. Ratings vary widely, often from 10% to 100%, depending on the anatomical level, major or minor extremity, loss of use, prosthetic function, and whether Special Monthly Compensation applies. Veterans should make sure VA evaluates not only the amputation but also functional loss, prosthetic limitations, pain, and SMC entitlement.
52. Amyotrophic Lateral Sclerosis (ALS)
Amyotrophic lateral sclerosis, or ALS, is a progressive neurological disease that affects motor neurons and causes worsening muscle weakness. It can affect movement, walking, speech, swallowing, breathing, and the ability to perform daily activities.
VA rates ALS under DC 8017 at 100%. VA should also consider Special Monthly Compensation where warranted, including loss of use, aid and attendance, respiratory impairment, and other serious residuals. ALS claims require careful attention to all complications and the veteran’s need for assistance.
53. Bladder Cancer
Bladder cancer is a malignant growth in the bladder. Veterans may claim bladder cancer based on direct service connection, toxic exposure, presumptive rules, or other service-related evidence.
VA rates active malignant genitourinary cancer under DC 7528 at 100%. After treatment ends, the 100% rating generally continues until mandatory review, and if there is no recurrence or metastasis, VA rates residuals such as voiding dysfunction or renal dysfunction. Evidence should document active disease, treatment, recurrence monitoring, urinary leakage, frequency, obstruction, infections, and kidney impact.
54. Blindness in One or Both Eyes
Blindness involves severe loss of vision in one or both eyes. It can result from trauma, disease, diabetes, toxic exposure, neurological injury, infection, or complications of another service-connected condition.
VA rates blindness under visual acuity, visual field, and anatomical loss criteria. Ratings can range from 0% to 100%, depending on objective testing, whether one or both eyes are affected, whether there is anatomical loss, and whether Special Monthly Compensation applies. Eye exams, visual field testing, specialist records, and functional evidence are critical.
55. Brain Disease Due to Trauma
Brain disease due to trauma generally refers to residuals of traumatic brain injury or other brain injury caused by head trauma. Symptoms can include memory problems, headaches, dizziness, balance problems, sleep impairment, mood changes, seizures, sensory issues, and cognitive dysfunction.
VA usually rates brain disease due to trauma as TBI under DC 8045. The TBI evaluation uses cognitive, emotional or behavioral, and physical facets, and may result in 0%, 10%, 40%, 70%, or 100%. Separate ratings may apply for distinct residual diagnoses, but VA cannot compensate the same symptom twice.
56. Chronic Headaches
Chronic headaches are recurrent headaches that may not meet the full diagnostic criteria for migraines but still cause pain, functional impairment, and disruption to daily life. They may be associated with TBI, neck conditions, sinusitis, sleep disorders, tinnitus, stress, or medication side effects.
VA commonly rates chronic headaches by analogy to migraines under DC 8100 at 0%, 10%, 30%, or 50%. Ratings depend on frequency, severity, prostrating attacks, duration, and economic impact. A headache log is one of the best forms of lay evidence because it can show how often headaches occur and how they affect work and daily activities.
Chronic inflammatory demyelinating polyneuropathy, or CIDP, is an immune-mediated neurological disorder that damages peripheral nerves. It can cause weakness, numbness, tingling, burning pain, balance problems, falls, reduced reflexes, fatigue, and difficulty walking or using the hands.
There is no single universal VA diagnostic code for CIDP. VA rates the condition by the affected peripheral nerve or nerves, and ratings vary based on incomplete or complete paralysis, motor loss, sensory loss, atrophy, and functional impairment. Neurology records, EMG or nerve conduction studies, reflex testing, strength testing, and limb-specific findings are important.
58. Chronic Liver Disease Due to Hepatitis C
Chronic liver disease due to hepatitis C occurs when hepatitis C causes ongoing liver inflammation, damage, or complications. Symptoms can include fatigue, malaise, nausea, anorexia, weight loss, abdominal pain, itching, joint pain, jaundice, and liver enlargement.
VA tracks hepatitis C under DC 7354 and evaluates it using the chronic liver disease criteria. Ratings can include 0%, 20%, 40%, 60%, or 100%, depending on severity, treatment, fatigue, malaise, anorexia, weight loss, hepatomegaly, pruritus, arthralgia, and medication or therapy requirements. Veterans should submit liver labs, imaging, hepatology records, treatment history, and complications.
59. Chronic Obstructive Pulmonary Disease (COPD)
COPD is a chronic lung disease that makes breathing difficult and can include chronic bronchitis, emphysema, or other airflow limitation. Veterans may claim COPD based on toxic exposure, burn pits, smoke, chemicals, occupational exposure, or aggravation during service.
VA rates COPD under DC 6604 at 10%, 30%, 60%, or 100%. Ratings are based primarily on pulmonary function tests, including FEV-1, FEV-1/FVC, DLCO, exercise capacity, oxygen therapy, cor pulmonale, pulmonary hypertension, right ventricular hypertrophy, and respiratory failure. Pulmonology records and valid PFT results are critical.
60. Chronic Pancreatitis
Chronic pancreatitis is long-term inflammation of the pancreas. It can cause abdominal or mid-back pain, nausea, vomiting, weight loss, greasy stools, diarrhea, bloating, maldigestion, malabsorption, and need for pancreatic enzymes.
VA rates chronic pancreatitis under DC 7347 at 30%, 60%, or 100%. Ratings depend on episodes of abdominal or mid-back pain, hospitalizations, outpatient treatment, complications, maldigestion, malabsorption, dietary restriction, and pancreatic enzyme supplementation. Diagnostic studies, hospital records, GI treatment notes, diet restrictions, and enzyme prescriptions are important evidence.
61. Chronic Renal Failure Requiring Dialysis
Chronic renal failure is severe kidney dysfunction, and regular dialysis indicates a very serious disability picture. Symptoms can include fatigue, swelling, nausea, weakness, shortness of breath, high blood pressure, reduced urination, itching, confusion, and dialysis dependence.
VA rates chronic renal disease requiring regular dialysis under DC 7530 as renal dysfunction. Regular dialysis supports a 100% rating, while other renal dysfunction levels can be 0%, 30%, 60%, 80%, or 100%, depending on GFR, albuminuria, edema, hypertension, and kidney function. Dialysis records, nephrology notes, labs, GFR results, and complication records should be submitted.
62. Chronic Skin Conditions
Chronic skin conditions include long-term dermatitis, rashes, infections, lesions, inflammatory skin disease, or other recurring skin problems. These conditions may flare due to heat, sweat, shaving, chemicals, uniforms, deployment exposure, environmental irritants, or stress.
VA rates chronic skin conditions under the specific skin diagnostic code, often using the General Rating Formula for the Skin. Common ratings are 0%, 10%, 30%, or 60%, based on body area affected and the type and duration of therapy, including topical or systemic treatment. Photos during flare-ups and treatment records are essential because skin conditions are often underrated when the exam happens on a good day.
63. Chronic Venous Insufficiency
Chronic venous insufficiency occurs when leg veins do not return blood properly to the heart. It can cause leg swelling, aching, heaviness, fatigue, visible veins, skin discoloration, eczema, ulcers, and pain that may improve with elevation or compression.
VA usually rates chronic venous insufficiency by analogy to DC 7121 or DC 7120 at 0%, 10%, 20%, 40%, 60%, or 100% per affected extremity. Ratings depend on edema, stasis pigmentation, eczema, ulceration, subcutaneous induration, and constant pain at rest. Each leg may be rated separately if both are affected.
64. Cirrhosis of the Liver
Cirrhosis is advanced scarring of the liver caused by chronic liver damage. It can result from hepatitis, toxic exposure, alcohol-related disease, fatty liver disease, autoimmune liver disease, or other causes.
VA rates cirrhosis of the liver under DC 7312 at 0%, 10%, 30%, 60%, or 100%. Ratings are based on liver disease severity, MELD score, portal hypertension, ascites, encephalopathy, variceal bleeding, weakness, anorexia, abdominal pain, and malaise. Hepatology records, imaging, labs, hospitalizations, MELD scores, and procedure records are important.
65. Degenerative Joint Disease
Degenerative joint disease is another term often used for osteoarthritis or joint degeneration. It commonly affects knees, hips, shoulders, ankles, hands, and the spine, causing pain, stiffness, swelling, reduced motion, crepitus, weakness, instability, and flare-ups with use.
VA usually rates degenerative joint disease under DC 5003 or the specific joint’s limitation-of-motion code. Ratings vary by joint, but x-ray-confirmed arthritis with painful or limited motion can support a compensable evaluation. Evidence should document the specific joint, imaging findings, pain, range of motion, flare-ups, and functional loss.
66. Excessive Tearing of the Eye
Excessive tearing involves dysfunction of the lacrimal apparatus, which produces or drains tears. It can result from trauma, surgery, chronic irritation, nerve problems, eye disease, or environmental exposure.
VA rates disorders of the lacrimal apparatus under DC 6025 at 10% for one eye or 20% for both eyes. Evidence should document whether one or both eyes are affected, chronicity, diagnosis, treatment, and how tearing affects vision, reading, driving, work, or daily activities.
67. Female Sexual Arousal Disorder
Female sexual arousal disorder involves impaired sexual arousal or response that causes distress or functional impact. It may be linked to trauma, medications, mental health conditions, neurological conditions, gynecological conditions, or other service-connected disabilities.
VA rates female sexual arousal disorder under DC 7632 at 0% schedularly. VA should review for entitlement to Special Monthly Compensation where applicable. Evidence should document diagnosis, symptoms, cause or aggravation, and the relationship to military service or a service-connected condition.
68. Gulf War Syndrome
Gulf War syndrome is a broad term often used for chronic unexplained symptoms in Gulf War veterans. These symptoms may involve fatigue, headaches, joint pain, muscle pain, skin symptoms, sleep problems, gastrointestinal symptoms, respiratory symptoms, neurological symptoms, and cognitive complaints.
There is no single diagnostic code for Gulf War syndrome. VA rates the actual diagnosed or undiagnosed manifestations, such as chronic fatigue syndrome, fibromyalgia, IBS, headaches, joint pain, skin symptoms, respiratory symptoms, or neurological symptoms. The claim is stronger when each manifestation is clearly documented with chronicity, severity, and functional impairment.
69. Hypertensive Vascular Disease
Hypertensive vascular disease generally refers to disability related to chronic high blood pressure and vascular effects. It may overlap with hypertension or hypertensive heart disease depending on the predominant condition.
VA usually rates hypertensive vascular disease under DC 7101 for hypertension at 10%, 20%, 40%, or 60%. If the predominant condition is hypertensive heart disease, VA may rate it under DC 7007 using the heart rating formula at 10%, 30%, 60%, or 100%. Evidence should clarify whether the disability is primarily blood pressure elevation, heart involvement, or both.
70. Hyperthyroidism
Hyperthyroidism occurs when the thyroid produces too much thyroid hormone. Symptoms can include weight loss, rapid heartbeat, palpitations, sweating, heat intolerance, tremors, anxiety, irritability, fatigue, and eye symptoms.
VA rates hyperthyroidism under DC 7900 at 30% for six months after initial diagnosis. After that, VA rates residuals such as cardiac, eye, endocrine, or other complications under the appropriate diagnostic code. Veterans should document diagnosis date, treatment, thyroid labs, residuals, and any ongoing heart, eye, weight, or mental health effects.
71. Impaired Vision
Impaired vision includes reduced visual acuity, visual field loss, double vision, eye muscle dysfunction, or other visual impairment. It can result from trauma, disease, diabetes, neurological injury, toxic exposure, or complications of another service-connected condition.
VA rates impaired vision under visual acuity, visual field, and muscle function criteria. Ratings can range from 0% to 100%, depending on objective eye testing, whether one or both eyes are service connected, and whether there is anatomical loss or severe impairment. Eye exams, visual field testing, specialist records, and functional evidence are critical.
72. Inflammation of a Nerve or Nerve Group
Inflammation of a nerve or nerve group, often called neuritis, involves irritation or inflammation of a peripheral or cranial nerve. Symptoms may include burning pain, shooting pain, numbness, tingling, weakness, reduced reflexes, muscle loss, and functional impairment.
VA rates neuritis under the affected nerve code. Ratings vary by nerve and severity, and VA considers sensory loss, pain, reflex changes, motor loss, atrophy, and whether impairment is mild, moderate, severe, or complete. The evidence should identify the nerve, side, severity, objective findings, and functional limitations.
73. Intervertebral Disc Syndrome (IVDS)
Intervertebral disc syndrome involves disc disease that causes acute episodes of symptoms due to herniation, nerve irritation, or spinal pathology. Symptoms may include back pain, neck pain, radiating pain, numbness, tingling, weakness, and severe flare-ups.
VA rates IVDS under DC 5243 either under the General Rating Formula for the Spine or under the Formula for Rating IVDS Based on Incapacitating Episodes, whichever results in the higher evaluation. IVDS episode ratings are 10%, 20%, 40%, or 60%, based on the total duration of physician-prescribed bed rest during the past 12 months. Self-imposed bed rest does not meet the IVDS definition.
74. Iron Deficiency Anemia
Iron deficiency anemia occurs when the body lacks enough iron to produce healthy red blood cells. Symptoms may include fatigue, weakness, shortness of breath, dizziness, headaches, pale skin, restless legs, rapid heartbeat, and reduced endurance.
VA rates iron deficiency anemia under DC 7720 at 0%, 10%, or 30%. The rating depends on whether the condition is asymptomatic or controlled by diet, requires continuous oral supplementation, or requires IV iron infusions. Evidence should include CBC results, ferritin, iron studies, oral supplement history, IV infusion records, and the underlying cause.
75. Labyrinthitis
Labyrinthitis is inflammation or dysfunction of the inner ear affecting balance and sometimes hearing. Symptoms can include dizziness, vertigo, imbalance, nausea, vomiting, hearing changes, tinnitus, and difficulty walking safely.
VA usually rates labyrinthitis as a peripheral vestibular disorder under DC 6204 at 10% for occasional dizziness and 30% for dizziness with occasional staggering. Hearing impairment or suppuration may be rated separately when appropriate. ENT records, vestibular testing, fall history, and symptom logs can help prove severity.
76. Loss of One Eye
Loss of one eye involves anatomical loss or severe functional impairment of one eye. It can result from trauma, disease, surgery, toxic exposure, infection, or complications of another service-connected condition.
VA rates loss of one eye under visual impairment and anatomical loss criteria. Anatomical loss of one eye may rate from about 40% to 100%, depending on impairment in the other eye and whether Special Monthly Compensation applies. Evidence should document anatomical loss, remaining eye function, prosthetic issues, depth perception problems, safety limitations, and functional impact.
77. Loss of Smell or Taste
Loss of smell or taste can occur after TBI, nasal injury, sinus disease, toxic exposure, neurological injury, infection, or other service-related conditions. It can affect appetite, safety, nutrition, and quality of life.
VA rates complete loss of smell under DC 6275 at 10% and complete loss of taste under DC 6276 at 10%. An anatomical or pathological basis is required. Objective medical evidence and a clear diagnosis are important because partial loss may not meet the compensable rating criteria.
78. Loss of Teeth
Loss of teeth can be compensable when due to loss of substance of the maxilla or mandible from trauma or qualifying disease, not ordinary periodontal disease. This is one of the most misunderstood VA disability claims because missing teeth alone do not automatically equal compensation.
VA rates loss of teeth under DC 9913 at 0%, 10%, 20%, 30%, or 40%. Ratings depend on the teeth lost, whether the masticatory surface can be restored by suitable prosthesis, and whether tooth loss is due to loss of substance of the maxilla or mandible. Dental trauma records, imaging, oral surgery records, and prosthetic evidence are important.
79. Lyme Disease
Lyme disease is an infectious disease transmitted by ticks. Veterans may claim Lyme disease based on field training, outdoor duty, deployments, or service environments where tick exposure occurred.
VA rates active Lyme disease under DC 6319 using the infectious disease formula, generally at 100% when active. After active disease resolves, VA rates residuals such as arthritis, Bell’s palsy, radiculopathy, ocular problems, or cognitive dysfunction under the appropriate body system. Evidence should include diagnosis, treatment, service exposure history, and chronic residuals.
80. Malaria
Malaria is an infectious disease transmitted by mosquitoes and may occur after service in endemic regions. Symptoms can include fever, chills, sweating, fatigue, headaches, muscle aches, nausea, anemia, and relapse episodes.
VA rates active malaria under DC 6304 at 100%. After active disease resolves, VA rates residuals such as liver, spleen, blood, neurological, or other organ complications under the appropriate body-system code. Diagnosis, deployment history, treatment records, lab confirmation, relapse history, and residual organ complications matter.
81. Malignant Growths of the Genitourinary System
Malignant growths of the genitourinary system include cancers affecting the bladder, prostate, kidney, testes, or other genitourinary structures. Symptoms can include urinary problems, blood in urine, pelvic pain, flank pain, fatigue, weight loss, sexual dysfunction, and treatment side effects.
VA rates active malignant genitourinary neoplasms under DC 7528 at 100%. After treatment and mandatory review, if there is no local recurrence or metastasis, VA rates residuals such as voiding dysfunction or renal dysfunction. Evidence should document diagnosis, active treatment, recurrence status, urinary leakage, frequency, kidney problems, erectile dysfunction, scars, and pain.
82. Malunion of the Lower Jaw
Malunion of the lower jaw occurs when the mandible heals improperly after fracture, trauma, or injury. It can cause jaw pain, open bite, chewing difficulty, malocclusion, clicking, popping, facial pain, and limited jaw function.
VA rates malunion of the mandible under DC 9904 at 0%, 10%, or 20%, based on displacement and open bite severity. Dental records, oral surgery notes, imaging, bite analysis, jaw measurements, and provider statements explaining chewing or speech impairment are important evidence.
83. Multiple Sclerosis
Multiple sclerosis is a chronic neurological disease where the immune system attacks the central nervous system. Symptoms can include weakness, numbness, vision problems, balance issues, tremors, bladder dysfunction, gait problems, fatigue, pain, and cognitive symptoms.
VA rates multiple sclerosis under DC 8018 with a minimum rating of 30%. VA can separately evaluate residuals such as vision impairment, bladder dysfunction, gait disturbance, weakness, fatigue, balance problems, and neurological impairment, which may combine higher, including to 100%. The key is identifying every residual and documenting its severity.
84. Muscle Spasms
Muscle spasms are involuntary muscle contractions that can be painful and functionally limiting. They often occur with spine conditions, muscle injuries, nerve irritation, overuse, joint disorders, or chronic musculoskeletal problems.
There is no standalone universal diagnostic code for muscle spasms. VA rates the underlying cause, such as a spine disability, muscle injury, joint condition, or nerve impairment. In spine claims, muscle spasm or guarding severe enough to result in abnormal gait or abnormal spinal contour can support a 20% spine rating. Evidence should document frequency, severity, abnormal gait, guarding, and functional loss.
85. Myasthenia Gravis
Myasthenia gravis is a chronic autoimmune neuromuscular disorder that causes muscle weakness. Symptoms often worsen with activity and may include drooping eyelids, double vision, swallowing problems, speech issues, breathing difficulty, fatigue, and limb weakness.
VA rates myasthenia gravis under DC 8025 with a minimum rating of 30%. VA can rate residuals separately, including vision, swallowing, speech, breathing, limb weakness, and fatigue, which can combine higher, including to 100%. The evidence should identify every affected body system and explain how symptoms impair daily function.
86. Neuralgia
Neuralgia is nerve pain caused by irritation or damage to a cranial or peripheral nerve. Symptoms may include sharp pain, burning pain, electric shock sensations, tingling, sensitivity to touch, numbness, and functional limitations.
VA rates neuralgia under the affected nerve’s neuralgia code, usually in the 87xx series. The maximum rating is generally equivalent to moderate incomplete paralysis of the affected nerve, except certain cranial nerve conditions such as tic douloureux may be rated higher. The evidence should identify the nerve and describe the distribution, severity, and functional impact of pain.
87. Neurogenic Bladder
Neurogenic bladder occurs when nerve problems interfere with bladder control. It can result from spinal cord injury, TBI, multiple sclerosis, diabetes, radiculopathy, or other neurological conditions.
VA rates neurogenic bladder under DC 7542 as voiding dysfunction or urinary tract infection, whichever is predominant. Voiding dysfunction can rate 20%, 40%, or 60%; urinary frequency can rate 10%, 20%, or 40%; and obstructed voiding can rate 0%, 10%, or 30%. Veterans should document leakage, pad use, frequency, nighttime urination, catheter use, infections, and retention.
88. Non-Hodgkin’s Lymphoma
Non-Hodgkin’s lymphoma is a cancer of the lymphatic system. Veterans may claim it based on direct service connection, Agent Orange exposure, toxic exposure, or other service-related evidence.
VA rates non-Hodgkin’s lymphoma under DC 7715 at 100% when there is active disease, during treatment, or with certain indolent and non-contiguous low-grade disease. After treatment and mandatory review, VA rates residuals. Evidence should document active disease, treatment, remission status, recurrence monitoring, fatigue, neuropathy, immune problems, organ damage, and mental health effects.
89. Paralysis of the Anterior Crural Nerve
Paralysis of the anterior crural nerve, also called the femoral nerve, affects the front of the thigh and quadriceps function. It may result from lumbar spine disease, trauma, surgery, diabetes, neuropathy, or nerve injury.
VA rates femoral or anterior crural nerve paralysis under DC 8526 at 10%, 20%, 30%, or 40%. Ratings are based on mild, moderate, severe incomplete paralysis, or complete paralysis of the quadriceps extensor muscles. Evidence should document thigh pain, numbness, weakness, knee extension problems, falls, and difficulty climbing stairs.
90. Paralysis of the Median Nerve
Paralysis of the median nerve affects wrist and hand function and is commonly associated with carpal tunnel syndrome, trauma, cervical radiculopathy, or nerve injury. Symptoms can include numbness, tingling, hand weakness, thumb weakness, grip problems, dropping objects, wrist pain, and impaired fine motor skills.
VA rates median nerve paralysis under DC 8515 from 10% to 70%, depending on severity and whether the major or minor hand is affected. Complete paralysis is rated 70% for the major hand and 60% for the minor hand. Evidence should document hand dominance, sensory symptoms, motor weakness, grip strength, EMG findings, and functional loss.
91. Parkinson’s Disease
Parkinson’s disease is a progressive neurological disorder that affects movement and can also cause cognitive, mood, sleep, speech, swallowing, bladder, and balance problems. It is a presumptive condition for certain exposed veterans.
VA rates Parkinson’s disease under DC 8004 with a minimum rating of 30%. VA can rate residuals separately, including tremors, gait impairment, balance problems, speech problems, swallowing issues, cognitive impairment, bladder dysfunction, mental health symptoms, and loss of use, which can combine higher, including to 100%. The 30% minimum is only the starting point.
92. Penile Deformity
Penile deformity may involve anatomical changes, Peyronie’s disease, trauma residuals, deformity associated with erectile dysfunction, or loss or removal of part of the penis under separate codes. Symptoms may include curvature, deformity, pain, erectile dysfunction, sexual dysfunction, and emotional distress.
Under current VA rules, erectile dysfunction with or without penile deformity is usually rated under DC 7522 at 0% schedularly, with possible entitlement to Special Monthly Compensation for loss of use of a creative organ. Anatomical loss or removal of part of the penis may be rated under separate diagnostic codes and may rate higher. Evidence should document diagnosis, anatomy, ED, cause, and SMC entitlement.
93. Peripheral Artery Disease
Peripheral artery disease is a vascular condition where narrowed arteries reduce blood flow, most often to the legs. Symptoms can include leg pain with walking, cramping, cold feet, numbness, slow-healing wounds, ulcers, skin changes, and reduced pulses.
VA rates peripheral artery disease under DC 7114 at 20%, 40%, 60%, or 100% per affected extremity. Ratings are based on objective vascular testing such as ABI, ankle pressure, toe pressure, and transcutaneous oxygen tension, along with functional impact. Vascular studies, surgical records, wound care records, and walking limitation evidence are important.
94. Residuals of Foot Injury
Residuals of foot injury refer to ongoing problems after a foot fracture, crush injury, sprain, strain, surgery, or other trauma. Symptoms may include foot pain, swelling, weakness, instability, altered gait, difficulty standing, difficulty walking, and reduced weight-bearing.
VA rates residuals of foot injury under DC 5284 at 10% for moderate, 20% for moderately severe, 30% for severe, and 40% with actual loss of use of the foot. The words moderate, moderately severe, and severe should be supported with real-world evidence, including walking limits, assistive devices, gait changes, pain with use, and work impact.
95. Sarcoidosis
Sarcoidosis is an inflammatory disease that can affect the lungs, lymph nodes, skin, eyes, heart, and other organs. Pulmonary involvement is common and may cause shortness of breath, cough, chest pain, fatigue, fever, night sweats, weight loss, skin lesions, eye symptoms, and joint pain.
VA rates sarcoidosis under DC 6846 at 0%, 30%, 60%, or 100%. Ratings are based on pulmonary involvement, corticosteroid treatment, cor pulmonale, cardiac involvement, fever, night sweats, weight loss, and progressive disease. VA may also rate sarcoidosis as chronic bronchitis or by residuals when appropriate.
96. General Scars
General scars include surgical scars, laceration scars, trauma scars, and other non-burn scars. VA evaluates scars based on pain, instability, size, depth, location, disfigurement, underlying soft tissue damage, and functional limitation.
VA rates scars under DC 7800, 7801, 7802, 7804, and 7805. Ratings can range from 0% to 80%, depending on whether scars are painful, unstable, disfiguring, deep, large, located on the head, face, or neck, or cause functional impairment. Painful or unstable scars under DC 7804 can rate 10%, 20%, or 30%, depending on the number of qualifying scars.
97. Seizure Disorders
Seizure disorders involve abnormal electrical activity in the brain that causes major or minor seizures. They may be related to TBI, neurological disease, infection, toxic exposure, or other service-connected conditions.
VA rates seizure disorders under DC 8910 through DC 8914 at 10%, 20%, 40%, 60%, 80%, or 100%. Ratings are based on the frequency of major and minor seizures, and continuous medication generally supports at least 10%. A seizure log, witness statements, ER records, medication history, and neurologist records are critical evidence.
98. Systemic Lupus Erythematosus
Systemic lupus erythematosus, or lupus, is an autoimmune disease that can affect joints, skin, kidneys, blood, lungs, heart, brain, and other organs. Symptoms may include fatigue, joint pain, rash, fever, photosensitivity, mouth sores, kidney problems, chest pain, anemia, and flare-ups.
VA rates systemic lupus erythematosus under DC 6350 at 10%, 60%, or 100%, or VA may separately rate residuals under the affected body systems if that produces a higher evaluation. Evidence should document flare frequency, systemic symptoms, medications, organ involvement, hospitalizations, and every affected body system.
99. Thigh Conditions
Thigh conditions include hip and thigh limitation of motion, impairment, pain, weakness, injury residuals, and functional limitations affecting walking, standing, sitting, climbing, or squatting. These conditions may result from trauma, arthritis, overuse, muscle injury, nerve problems, or service-connected hip and spine conditions.
VA rates thigh conditions under the specific hip or thigh diagnostic code. Common codes include DC 5251 for extension limited to 5 degrees at 10%, DC 5252 for flexion limitation at 10%, 20%, 30%, or 40%, and DC 5253 for impairment of thigh at 10% or 20%. More severe hip or femur conditions may rate higher under other codes. Range of motion, pain, flare-ups, gait changes, and functional loss should be documented.
100. Thyroid Cancer
Thyroid cancer is a malignant endocrine neoplasm affecting the thyroid gland. Veterans may claim thyroid cancer based on radiation exposure, toxic exposure, direct service connection, or other service-related evidence.
VA rates active thyroid cancer under DC 7914 at 100%. After treatment and required review, if there is no recurrence or metastasis, VA rates residuals under the appropriate body system. Residuals may include hypothyroidism, voice changes, swallowing problems, scars, fatigue, hormone replacement needs, and other endocrine or surgical effects.
Content Reviewed By
Quality Assurance Team
The Quality Assurance (QA) team at VA Claims Insider has extensive experience researching, fact-checking, and ensuring accuracy in all produced content. The QA team consists of individuals with specialized knowledge in the VA disability claims adjudication processes, laws and regulations, and they understand the needs of our target audience. Any changes or suggestions the QA team makes are thoroughly reviewed and incorporated into the content by our writers and creators.
Brian Reese is a world-renowned VA disability benefits expert and the #1 bestselling author of VA Claim Secrets and You Deserve It. Motivated by his own frustration with the VA claim process, Brian founded VA Claims Insider to help disabled veterans secure their VA disability compensation faster, regardless of their past struggles with the VA. Since 2013, he has positively impacted the lives of over 10 million military, veterans, and their families.
A former active-duty Air Force officer, Brian has extensive experience leading diverse teams in challenging international environments, including a combat tour in Afghanistan in 2011 supporting Operation ENDURING FREEDOM.
Brian is a Distinguished Graduate of Management from the United States Air Force Academy and earned his MBA from Oklahoma State University’s Spears School of Business, where he was a National Honor Scholar, ranking in the top 1% of his class.
On June 10, 2026, VA announced it had processed more than 2 million disability benefits claims in fiscal year 2026 as of June 1. That’s a record, and to be fair, it’s a big deal. Or is it?
VA also reported that it has already awarded more than $124 billion in compensation and pension benefits to veterans and survivors this fiscal year. The average time to complete a claim decision is now 78.6 days, down from 141.5 days on January 20, 2025. That’s almost 2X faster.
I’ll give credit where credit is due: veterans deserve faster VA rating decisions. Nobody should have to wait months or years for benefits they earned through honorable service to our country. Faster claims processing is a good thing.
But faster doesn’t always mean better.
A fast approval with the correct rating and effective date is great. But a fast denial is still a denial. A fast lowball rating is still a lowball rating. A fast decision based on a bad C&P exam is still a bad decision. And a fast VA mistake can still cost a veteran and their family thousands of dollars in tax-free compensation and potentially years of struggle.
That’s the part that gets lost in the headline.
VA is celebrating speed, and I get it. Speed matters. But veterans don’t just need fast decisions. Veterans need accurate decisions. They need the correct rating percentage, the correct effective date, and the correct monthly compensation. That’s the real scoreboard.
Table of Contents
Summary of Key Points
VA processing 2 million disability claims in record time is good news, but faster doesn’t always mean better. Veterans don’t just need quick decisions—they need accurate decisions with the correct rating, effective date, and monthly compensation.
VA’s 94% accuracy claim lacks real-world context. Veterans deserve more transparency on denial rates, lowball ratings, bad C&P exams, effective date errors, and how many “completed” claims later get fixed on appeal.
A faster VA system can deny or lowball weak claims faster. If your claim is missing medical evidence, lacks a clear nexus, has undocumented symptoms, or you’re unprepared for your C&P exam, speed can work against you.
The best way to win your VA claim is to build it right before you file using the VA Claims Insider Golden Circle and SEM Method: current diagnosis, in-service event, nexus, severity of symptoms, plus Strategy, Education, and Medical Evidence.
The VA Announcement Lacks Context
VA says claims processing accuracy are currently above 94%. That would mean 94/100 VA rating decision were accurate. In my experience, there’s no way that’s correct. I’d love to see more context behind that number and what it actually means. Data can be fudged to tell the story one wants to tell.
So when VA says, “We processed 2 million claims,” my response is simple: Great. Now show us how many were correct. Not just your bumper sticker number.
I’d love to see VA publish more data on denial rates, lowball ratings, effective date errors, bad C&P exams that ruin a claim, and how many veterans win later on Higher-Level Review, Supplemental Claim, Board appeal, or Court appeal. I’d also love to know how many “completed” claims are really just the beginning of another fight. Tell us how many veterans are losing or getting lowballed.
While speed matters, accuracy matters more.
A Faster VA Can Deny Weak Claims In Record Time
Here’s what every veteran needs to understand: a faster VA system can help you if your claim is strong, but it can hurt you if your claim is weak.
Sadly, in my experience, even if your claim is strong, human error or a bad C&P exam can blow it all up.
And if your claim is missing medical evidence, VA can deny it faster. If your symptoms aren’t documented, VA can lowball you faster. If you walk into your C&P exam unprepared, VA can make a bad decision faster. If you file the wrong condition the wrong way, VA can close your claim and move on faster.
Most veterans know exactly what happened to them in the military. They know what they went through, what hurts, what changed after service, and how bad their symptoms really are. They know how their disabilities affect their marriage, family, work, sleep, mood, body, and daily life.
But VA does not rate what you know or say. VA rates what the evidence shows.
Just like in the military, if it’s not written down on paper, it might as well not exist. That’s not fair, but it is reality. And once you understand that you can do something about it.
Don’t File and Hope
One of the biggest mistakes veterans make is filing a claim and hoping VA figures it out.
Hope is not a strategy.
VA raters are not mind readers. C&P examiners are not your friend. Nobody should care more about your claim than you do.
You need to build your claim before you file it, and that starts with what we call the VA Claims Insider Golden Circle.
Every strong VA disability claim needs four things: (1) a current diagnosis, (2) an in-service event, injury, disease, or aggravation, (3) a clear nexus for service connection, and (4) documented severity of symptoms.
The VA Claims Insider Golden Circle
The first thing you need is a current diagnosis in a medical record. Not just pain, not just symptoms, not just “I think I have it,” and not just because I wrote it in this personal statement. If you’re claiming migraines, PTSD, GERD, sleep apnea, depression, radiculopathy, sinusitis, IBS, or any other condition, where is it diagnosed in a medical record? Without a current diagnosis, VA has an easy reason to deny the claim. In fact, you might not even get scheduled for a C&P exam.
The second thing you need is evidence of an in-service event, injury, disease, or aggravation. This could be an injury, deployment, toxic exposure, traumatic event, training accident, combat event, military sexual trauma, physical wear and tear, or a condition that started or got worse in service. Sometimes that evidence is in your Service Treatment Records. Sometimes it’s in your DD214, personnel records, deployment records, lay statements, personal statement, awards and decorations, performance reports, newspaper clippings, a journal, etc. The point is simple: you need to be able to point back to something that happened in-service.
The third thing you need is a clear nexus, which simply means a link or connection. This is where a lot of veterans lose, especially those who have been out of the military for than 1 year. You can have a current diagnosis and something that happened in service, but if you can’t connect the two, VA can still deny your claim (and they probably will). For secondary claims, the nexus connects your new condition to a condition you’re already service connected for, such as migraines secondary to tinnitus, depression secondary to chronic pain, GERD secondary to PTSD medication, sleep apnea secondary to weight gain caused by a service-connected condition, or radiculopathy secondary to a back condition. This is why a strong private Nexus Letter can be a game changer when written correctly with high probative value.
The fourth thing you need is documentation of your severity of symptoms. This is what drives your final VA rating percentage. VA doesn’t rate you just because you have a condition; VA rates how bad the condition is. How often does it happen? How severe is it? How long does it last? How does it affect your work, life, and social functioning? This is where veterans get crushed. They minimize symptoms, talk about their best day, leave out the ugly stuff, and fail to explain how bad it really gets. Don’t do that. Tell the truth for sure—not the tough-guy version, not the cleaned-up version, but the real version. Be honest, be specific, and be uncomfortably vulnerable at your C&P exam.
The SEM Method Explained
At VA Claims Insider, we teach veterans the SEM Method:
Strategy + Education + Medical Evidence = VA Rating You Deserve
That’s it. Simple, but not always easy.
Strategy means you don’t throw 20 random conditions at VA and hope something sticks. That’s not a strategy; that’s a mess. More conditions can mean more exams, more confusion, more delays, more denials, and more chances for VA to get something wrong. A focused claim beats a messy claim. Before you file, ask yourself: What are my strongest claims? What conditions are diagnosed? What evidence do I already have? What evidence am I missing? Is this a direct, secondary, presumptive, aggravation, or increase claim? Will this condition actually move my combined rating? Do I need a DBQ or Nexus Letter? Is this claim ready to file?
Education means you don’t need to become a lawyer or a doctor, but you do need to understand the basics. You need to know how VA service connection works, how your condition is rated, what a C&P exam is really for, what a DBQ is, when a Nexus Letter matters, and how to read your VA decision letter. Once you understand the game, you can play it better.
Medical evidence is what wins VA claims. Period. Your evidence needs to prove the Golden Circle: diagnosis, in-service event, nexus, and severity. That evidence can include VA medical records, private medical records, Service Treatment Records, DBQs, Nexus Letters, Independent Medical Opinions, buddy statements, lay statements, sleep studies, imaging, labs, prescriptions, and mental health records. Do not make VA guess. Do not assume the rater will connect the dots. Do not assume the C&P examiner will tell your story correctly. They won’t. Make the evidence obvious.
Conclusion & Wrap-Up
VA processing 2 million claims in record time is good news, and I’m glad claims are moving faster. But veterans need more than fast. Veterans need accurate.
They need the correct rating, correct effective date, correct monthly compensation, and correct benefits for themselves and their families.
So my message to VA is simple: keep getting faster, but don’t sacrifice accuracy.
Be transparent and publish the bad along with the good because veterans deserve to know what’s really going on.
And my message to veterans is even simpler: don’t file a weak claim into a faster system because you’ll likely get crushed.
Build and file your own VA claim online the right way. Get a current diagnosis. Document the in-service event, injury, disease, or aggravation. Prove a clear nexus. Document the true severity of your symptoms. Use strategy, get educated, gather medical evidence, and prepare to crush your VA C&P exam.
And if VA gets it wrong, don’t quit.
A denial is not the end. A lowball rating is not the end. A bad C&P exam is not the end.
You Served. You Deserve.
Looking for VA Claim Help Fast? WE GOT YOUR SIX!
VA Claims Insider is the #1 most trusted name in VA disability claims.
Work 1:1 with a VA claims expert coach who can help lead you to VA claim victory.
50,000+ disabled veterans served in our membership programs since 2016.
33% average rating increase for veterans who complete our Elite program.
The Quality Assurance (QA) team at VA Claims Insider has extensive experience researching, fact-checking, and ensuring accuracy in all produced content. The QA team consists of individuals with specialized knowledge in the VA disability claims adjudication processes, laws and regulations, and they understand the needs of our target audience. Any changes or suggestions the QA team makes are thoroughly reviewed and incorporated into the content by our writers and creators.
Brian Reese is a world-renowned VA disability benefits expert and the #1 bestselling author of VA Claim Secrets and You Deserve It. Motivated by his own frustration with the VA claim process, Brian founded VA Claims Insider to help disabled veterans secure their VA disability compensation faster, regardless of their past struggles with the VA. Since 2013, he has positively impacted the lives of over 10 million military, veterans, and their families.
A former active-duty Air Force officer, Brian has extensive experience leading diverse teams in challenging international environments, including a combat tour in Afghanistan in 2011 supporting Operation ENDURING FREEDOM.
Brian is a Distinguished Graduate of Management from the United States Air Force Academy and earned his MBA from Oklahoma State University’s Spears School of Business, where he was a National Honor Scholar, ranking in the top 1% of his class.
Patellofemoral pain syndrome is typically rated from 0% to 50%, under the knee rating criteria, based on the symptoms and functional limitations you experience.
Dealing with chronic knee pain is a daily struggle. It hurts to climb stairs, squatting feels impossible, and your knees ache after sitting for long periods. If that sounds familiar, you may have patellofemoral pain syndrome (PFPS), sometimes called “runner’s knee,” and you may qualify for a VA rating and compensation.
Understanding your patellofemoral pain syndrome VA rating is important because the VA doesn’t assign ratings based on your diagnosis alone. Instead, your rating depends on how much the condition limits your function, range of motion, stability, and daily activities.
The good news is that even if imaging looks normal, you can still qualify for VA disability compensation if your symptoms are service-connected and properly documented.
Summary of Key Points
Patellofemoral pain syndrome (PFPS) is a common cause of chronic knee pain and is frequently service-connected by the VA.
There is no standalone diagnostic code for PFPS; the VA typically rates it based on limitation of motion, painful motion, instability, or other knee impairments.
Many veterans receive a minimum 10% rating for painful motion, even when range-of-motion loss is relatively mild.
Separate ratings may be available for instability, limitation of flexion, limitation of extension, and certain surgical residuals.
Strong medical evidence, lay statements, and an accurate compensation and pension (C&P) exam can significantly impact your rating.
Table of Contents
What is Patellofemoral Pain Syndrome?
Patellofemoral pain syndrome is a condition that causes pain around or behind the kneecap (patella). Medical experts describe it as one of the most common causes of anterior knee pain. Symptoms typically worsen during activities that place stress on a bent knee, including squatting, climbing stairs, running, kneeling, or prolonged sitting.
Some veterans also experience grinding, clicking, or popping sensations in the knee. While symptoms vary from person to person, the condition often interferes with daily activities that require bending or weight-bearing.
For many veterans, PFPS develops from years of:
Ruck marching
Running
Airborne operations
Repetitive kneeling
Physical training
Military occupational duties requiring prolonged standing or load-bearing
How the VA Rates Patellofemoral Pain Syndrome
The VA does not assign a disability rating based solely on a diagnosis of patellofemoral pain syndrome.
Instead, the condition is generally rated under the knee rating criteria found in 38 CFR § 4.71a, based on the symptoms and functional limitations you experience.
The VA commonly evaluates PFPS using:
Diagnostic Code (DC) 5260 – Limitation of flexion: 0%–30%
Diagnostic Code (DC) 5261 – Limitation of extension: 0%–50%
Service-connected but symptoms do not meet compensable criteria
10%
Painful motion or mild limitation of motion
20%
More significant limitation of flexion, extension, or instability
30%+
Severe limitation of motion, instability, or other qualifying knee impairment
A 10% evaluation is often assigned when patellofemoral pain syndrome causes painful motion but does not result in compensable limitation of flexion or extension under the knee rating criteria.
How Range of Motion Affects Your VA Rating
The VA pays close attention to range-of-motion measurements during your C&P examination.
Knee Flexion VA Ratings
Flexion refers to bending your knee.
The more limited your ability to bend the knee, the higher your potential rating.
Your examiner will measure:
Initial range of motion
Painful motion
Repetitive-use limitations
Flare-up limitations
Knee Extension Ratings
Extension refers to straightening your leg.
Veterans with significant extension limitations may qualify for ratings higher than those available solely for flexion loss.
Because PFPS symptoms often worsen during repetitive use, it’s important to accurately describe flare-ups, functional loss, daily limitations, and activity restrictions.
Never push through pain during range-of-motion testing simply to “look tough.”
Can You Receive Separate Ratings for the Same Knee?
Sometimes, yes.
Depending on the evidence, the VA may assign separate ratings for the different ways knee conditions present themselves.
In some situations, the VA can assign multiple ratings for the same knee when different symptoms are being compensated.
For example, a veteran may receive one rating for limited motion and another for instability if each condition creates a separate functional impairment. Additional ratings may also be available for certain meniscus injuries or painful surgical scars.
However, VA rules prohibit compensating the same symptom twice, a practice known as pyramiding.
This is one reason why a thorough review of your medical evidence can make a significant difference in your overall disability rating.
How to Prove Service Connection
Like most VA disability claims, a claim for patellofemoral pain syndrome generally requires three elements:
A current diagnosis, and
An in-service event, injury, illness, or aggravation, and
A medical nexus linking the two (e.g., a nexus letter)
The diagnosis may be provided by a VA provider, a private physician, an orthopedic specialist, or a physical therapist.
Evidence of an in-service event could include documented knee injuries, physically demanding military duties, airborne operations, or years of stress from training and occupational activities.
Finally, the VA must see evidence showing that your current condition is “at least as likely as not” related to your military service.
The knee C&P exam is often the most important part of your claim.
The examiner may evaluate:
Range of motion
Painful motion
Functional loss
Flare-ups
Instability
Use of braces or assistive devices
Occupational limitations
Before your exam, think about how your knee condition affects daily tasks such as walking, standing, climbing stairs, squatting, and work or home activities.
Be specific and accurate. The VA is evaluating functional impairment, not simply whether you have knee pain.
Can Patellofemoral Pain Syndrome Lead to Secondary VA Claims?
Absolutely.
Chronic knee pain rarely exists in isolation. When one knee becomes painful, many people unconsciously change the way they walk, stand, and distribute weight. Over time, these compensatory movements place additional stress on other joints and body systems.
If a service-connected knee condition causes or aggravates another disability, you may qualify for secondary service connection.
How to Strengthen a Patellofemoral Pain Syndrome VA Claim
The strongest claims typically include the strongest medical evidence.
In addition to a current diagnosis, in-service event, and a nexus connecting the two, consider submitting:
Any additional service treatment records or physical therapy records
Imaging studies
Personal/Buddy/Employer statements
Independent medical opinions
Your lay evidence should clearly explain:
When symptoms began
How symptoms progressed
Functional limitations
Impact on work and daily life
Specific examples are usually more persuasive than general statements.
When Should You File for an Increase?
You may want to seek an increased rating if:
Pain has worsened
Range of motion has decreased
Your knee gives out more frequently
You require braces or assistive devices
New secondary conditions have developed
Conclusion
A patellofemoral pain syndrome VA rating can range from 0% to 50% or higher, depending on how the condition affects your knee function, stability, and daily life.
The diagnosis itself doesn’t determine your rating; the severity of your symptoms does.
If your knee pain affects your ability to walk, squat, climb stairs, work, or stay active, make sure those limitations are clearly documented in your medical records and during your C&P exam.
The stronger your evidence, the stronger your claim.
FAQs | Frequently Asked Questions
What is the average patellofemoral pain syndrome VA rating?
Many veterans receive a 10% rating because painful motion can qualify for compensation even when range-of-motion limitations are relatively mild.
Is patellofemoral pain syndrome a disability for VA purposes?
Yes. If PFPS is service-connected and causes functional impairment, it may qualify for VA disability compensation.
Can I receive separate ratings for both knees?
Yes. If both knees are service connected, each knee is evaluated separately. The VA may also apply the bilateral factor when appropriate.
Can I get a VA rating for knee pain without arthritis?
Yes. Patellofemoral pain syndrome does not require an arthritis diagnosis. Functional loss and painful motion can support a compensable rating.
Can patellofemoral pain syndrome be secondary to another condition?
Yes. In some cases, PFPS may be caused or aggravated by service-connected foot, ankle, hip, or gait-related conditions.
What evidence helps increase a patellofemoral syndrome VA rating?
Strong evidence may include updated medical or physical therapy records, a credible nexus letter and DBQ, lay statements, independent medical opinions (IMOs), or documentation of flare-ups and functional loss.
Can I receive VA disability for patellofemoral pain syndrome in both knees?
Yes. Bilateral patellofemoral pain syndrome is common, and each knee may be rated separately if service connection is established. To calculate the bilator factor for VA disability compensation, see the VA Disability Calculator.
What We Believe
Our WHY
We believe millions of veterans feel overlooked, lowballed, denied, or lost in the VA claims process.
Our purpose is to help underrated disabled veterans rated 0% to 90% create real life change by pursuing the VA disability benefits they legally, morally, ethically, and medically deserve.
We are INSIDERS.
Our HOW
We make the VA disability process easier through expert-level education, proven resources, and veteran-to-veteran support.
You are never alone in this fight.
Our flagship program, VA Claims Insider Elite, connects each veteran with an expert-level Veteran Coach who guides them through our proprietary 8-step process.
That process is built around our SEM Method:
Strategy + Education + Medical Evidence = VA Rating You Deserve!
Our WHAT
We help underrated disabled veterans rated 0% to 90% win, service connect, and increase their VA rating through a smarter strategy, better education, and stronger medical evidence.
YOU SERVED. YOU DESERVE.
Do you have the VA rating you were given…or the VA rating you actually deserve?
Because getting a decision from the VA does not always mean you got the right decision from the VA.
If you are rated anywhere from 0% to 90% and feel stuck, frustrated, underrated, denied, or overlooked, I am speaking directly to you.
And if you have never filed because you thought other veterans deserved it more, because you got denied before, or because you assumed it was too late, do not let those myths make your decision for you.
At VA Claims Insider, we help underrated disabled veterans create real life change by getting the VA rating and compensation they deserve!
Here’s a sliver of what you get when you join us:
A Veteran Coach by your side, so you never have to fight the VA alone.
A smarter, personalized strategy for your claim.
Better VA disability education, so you know what to do next.
Stronger private medical evidence (DBQs, Nexus Letters, Mental Health Evaluations, and more) at members-only rates to support the rating you deserve.
And a proven battle plan toward VA claim victory.
But maybe you’re wondering: Will this actually work for me?
That is a fair question.
At VA Claims Insider, we have helped 50,000+ veterans fight for the VA disability benefits they earned.
Our internal data shows an average *33% VA rating increase for veterans who complete our Elite program.
Our internal data also shows veterans in our programs get their claims approved *25% faster on average than the VA’s published average claim-processing timelines.
Veterans in our community have left 7,000+ total reviews, with a 4.6 out of 5 average rating.
More than 5,500 reviews are 5 stars, and 92% of all veteran customer reviews are either 4 or 5 stars.
*Based on VA Claims Insider internal data for veterans who completed the Elite program. Average results shown; individual results vary. No guaranteed outcome or faster claim processing.
If you are ready for a better battle plan, a smarter strategy, and the right path to the VA rating and compensation you deserve, we’ve got your six.
Call us now at 737-295-2226 or click the red button below to get started:
Katie McCarthy is a writer and editor with experience in daily news and digital and print magazine publishing. She honed her editorial (and firearms) skills at Guns & Ammo before helping launch Black Rifle Coffee Company’s Coffee or Die Magazine as the managing editor. She holds degrees in English (BA) and public administration (MPA). Katie is a military spouse and word nerd who enjoys reading, hiking, camping, gardening, and spending time with her family.
New VA disability claims data reveals a brutal truth: Most veterans begin their VA disability journey underrated. The most common starting rating is 10%, but the most common rating overall is 100%.
That means many veterans don’t stay where VA first rated them—they keep fighting, building the right evidence, and proving what they deserved all along.
According to the newly released 2025 VBA Compensation Report, the most common combined VA disability rating for new compensation recipients in FY2025 was just 10%.
Let that sink in for a minute.
Of the 476,802 veterans who began receiving VA disability compensation in FY2025, 131,924 were rated 10%. That was the single most common rating for new recipients. Wowza.
But here’s where the data gets really interesting.
Among allveterans receiving VA disability compensation, the most common combined rating is now 100%.
For example, VA reported 1,847,449 veterans rated 100% in FY2025. That’s more than 29% of all veterans receiving VA disability compensation.
That is a massive gap and it begs the question: Why are so many veterans starting at 10%, while 100% is now the most common rating overall?
In my experience helping millions of veterans since 2013, this is one of the biggest warning signs in the entire report.
Millions of deserving veterans enter the VA claims process undereducated, underprepared, and underevidenced. They file a claim, guess their way through it, toss everything at the wall to see what sticks, minimize their symptoms, leave out high-value claims and secondary conditions, fail to fully explain functional impairment, and submit weak or incomplete evidence.
Then VA comes back with a denial, 0%, 10%, 30%, 50%, 70%, or a rating that does not reflect the full severity of what they’re dealing with. That’s usually when the light bulb turns on.
Veterans start asking themselves:
“Why did I get a lowball rating when my buddy is at 100%?”
“Did the VA miss something in my records/evidence?”
“Did I do something wrong that could have caused this?”
“Why do some conditions I filed for say not service connected?”
“Did I miss conditions I should have claimed?”
“What do I do now?”
Okay, let’s break down the most important trends from VA’s 2025 VBA Compensation Report and what they really mean for veterans.
Summary of Key Points
The most common new VA disability rating is 10%. VA’s 2025 data shows 131,924 new compensation recipients were rated 10%, making it the most common starting point for newly rated veterans.
100% is now the most common VA disability rating overall. Nearly 1.85 million veterans are rated 100%, representing more than 29% of all veterans receiving VA disability compensation.
The gap between 10% and 100% shows many veterans start underrated. A low rating does not always mean the condition is mild; sometimes it means VA did not have the full picture, including secondary conditions, functional impairment, and strong medical evidence.
Modern VA claims are rarely about one condition. VA reported more than 46.4 million service-connected disabilities across 6.3 million veterans, proving that strategy, education, and evidence are critical to getting the rating veterans legally deserve.
Table of Contents
Key Takeaways from the 2025 VBA Compensation Report
Data Point
2025 VBA Claims Data
Why It Matters
New veterans receiving VA compensation
476,802
Nearly half a million veterans newly entered the VA compensation system.
Most common new VA rating
10%
Many veterans start at the lowest compensable rating.
New recipients rated 10%
131,924
About 27.7% of all new recipients were rated 10%.
New recipients rated 100%
73,649
About 15.4% of new recipients started at 100%.
Total veterans receiving VA compensation
6,338,253
More than 6.3 million veterans now receive VA disability compensation.
Veterans rated 100% overall
1,847,449
Nearly 1.85 million veterans are now rated 100%.
Percent of all recipients rated 100%
29.15%
100% is now the most common combined rating overall.
Total service-connected disabilities
46,496,235
Modern VA claims are rarely about one simple condition.
Average disabilities per compensated veteran
7.34
The average compensated veteran has more than seven service-connected disabilities.
Average disabilities per new recipient
6.15
Even new recipients are entering the system with multiple rated conditions.
The Most Common New VA Disability Rating Is 10%
The biggest takeaway from the report is simple: The most common new VA disability rating is 10%.
That does not automatically mean VA got every rating wrong. But it should make veterans pay attention.
A 10% rating does not always mean your condition is mild. Sometimes it means VA did not have the full picture.
Maybe your service treatment records (STRs) were thin because you didn’t go to the doctor on active duty. Maybe you didn’t submit the right evidence. Maybe VA claims adjudicators missed some of your evidence. Maybe your C&P exam did not capture your worst symptoms. Maybe you did not explain functional impairment and how your condition affects your work, sleep, relationships, movement, focus, mood, or daily life.
Maybe you didn’t have a current diagnosis, evidence of an in-service event, injury, disease, or aggravation, a clear nexus for service connection, or documentation of your severity of symptoms.
This is where a lot of veterans get hurt. They assume VA will connect the dots for them.
Do not assume that.
VA rates what is in the record. If the evidence does not clearly show the severity of your condition, you can get underrated.
Pro Tip: A lowball VA rating should always lead to one question: Did VA have the full story? If VA did not have the full story, your rating may not reflect the full impact of your service-connected condition.
Nearly 1.85 Million Veterans Are Now Rated 100%
Now let’s look at the other side of the data.
VA reported 1,847,449 veterans rated 100% disabled in FY2025. That is the largest rating group among all veterans receiving VA disability compensation.
That is a big deal. But let me be very clear: This does not mean every veteran should be rated 100%.
It means more veterans are learning how to properly document the full impact of their service-connected disabilities.
Many veterans do not get the correct rating the first time. They learn the system. They file to increase their VA rating. They claim secondary conditions. They appeal bad decisions. They submit stronger medical evidence. They get better C&P exams. They stop minimizing their symptoms. They work with an expert.
And over time, their rating starts to better reflect reality.
That is the story buried inside this report. Many veterans start low because they do not know what they do not know.
The Number of 100% Rated Veterans Is Growing Fast
The 100% VA rating category is not just the largest rating group. It is also growing fast.
In FY2024, VA reported 1,547,842 veterans at 100%. In FY2025, that number jumped to 1,847,449.
That is an increase of 299,607 veterans in one year, or about a 19% increase.
Go back to FY2021, and VA reported 972,893 veterans rated 100%. That means the number of 100% rated veterans has nearly doubled in just four years.
Again, this does not mean every veteran qualifies for 100%. But it does tell us something important:
More veterans are documenting the true severity of their conditions.
More veterans are filing secondary claims.
More veterans are pursuing increases.
More veterans are appealing bad decisions.
More veterans are realizing the first rating VA gives them may not be the final answer.
Modern VA Claims Are Rarely About One Condition
This might be the most important data point in the entire report: VA reported 46,496,235 service-connected disabilities across 6,338,253 veterans receiving compensation.
That equals an average of 7.34 service-connected disabilities per veteran.
For new recipients, VA reported 2,933,013 service-connected disabilities across 476,802 veterans. That equals an average of 6.15 service-connected disabilities per new recipient.
Translation?
Today’s VA claims are not usually about one simple condition.
They are about multiple conditions, multiple body systems, secondary connections, worsening symptoms, overlapping impairments, and evidence that explains how all of it affects your life.
The 0% and 10% Trap
The report also shows something every veteran needs to understand.
A huge number of individual service-connected disabilities are rated 0% or 10%.
Together, that is more than 31 million individual service-connected disabilities rated either 0% or 10%.
That is massive.
Now, a 0% rating is not worthless. In many cases, it is very valuable because VA has granted service connection. But 0% also means VA is saying your condition does not meet the criteria for monthly compensation.
That might be correct. Or it might mean the evidence did not show the true severity of your symptoms.
Same thing with 10%. A 10% rating might be accurate. But it might also be a starting point.
What to Do If You Have a 0% or 10% Rating
Do not ignore it. Review it.
Read the VA rating decision letter.
Look at the evidence VA used.
Look at the rating criteria.
Ask whether the decision matches your actual symptoms.
Ask whether the condition has worsened.
Ask whether the condition caused or aggravated another condition.
Sometimes service connection is the hardest part. Once VA grants it, the next question becomes whether the rating is correct. You can always file for increases if your symptoms get worse.
10 Most Common VA Disability Claims Right Now
VA’s report also shows the most common service-connected disabilities among all veterans receiving compensation.
The top 10 were:
Tinnitus
Limitation of flexion, knee
Paralysis of the sciatic nerve
Lumbosacral or cervical strain
PTSD
Hearing loss
Limitation of motion of the arm
Scars and burns
Migraine
Limitation of motion of the ankle
These 10 conditions accounted for 18,448,237 service-connected disabilities, which is nearly 40% of all service-connected disabilities in the report.
For new recipients, the list was very similar:
Tinnitus
Limitation of flexion, knee
Lumbosacral or cervical strain
Limitation of motion of the arm
Hearing loss
Scars and burns
Migraine
Paralysis of the sciatic nerve
PTSD
Limitation of motion of the ankle
The takeaway is simple: The most common VA claims are heavily concentrated in hearing conditions, joint and spine conditions, nerve issues, migraines, scars, and mental health.
If you are a veteran dealing with these conditions, you are not alone. But common does not mean automatic. You still need the right evidence.
Musculoskeletal Conditions Dominate VA Claims
Musculoskeletal conditions are the biggest category of VA disability claims by far.
VA reported 17,838,998 musculoskeletal service-connected disabilities, which represented 38.4% of all service-connected disabilities.
This includes conditions involving the knees, back, neck, shoulders, ankles, hips, feet, and other joints.
Here is the problem: Musculoskeletal claims are often underrated when veterans fail to properly explain functional loss.
VA is not just looking for pain. VA is looking at how the condition affects movement and function.
That means things like:
Painful motion
Flare-ups
Range of motion
Repeated use over time
Difficulty standing
Difficulty walking
Difficulty lifting
Difficulty bending
Difficulty sitting
Difficulty using stairs
Impact on work and daily life
Too many veterans walk into a C&P exam on a “good day,” push through the pain, and say, “I’m fine.”
Do not do that.
Tell the truth. Explain your worst days. Explain what happens after repeated use. Explain how flare-ups affect you. Explain what you can no longer do.
That is not complaining. That is evidence.
Mental Health Claims Are Different
One of the most important hidden gems in the report is the mental health data.
VA reported 3,163,838 mental health service-connected disabilities.
The most common mental health rating was 70%, making it a high-value claim.
That matters.
Mental health claims are rated based on occupational and social impairment. That means VA is looking at how your symptoms affect your ability to work, function, maintain relationships, handle stress, control emotions, sleep, focus, and live your life.
PTSD was the most common mental health condition in the report, with 1,760,497 service-connected PTSD disabilities. That represented 55.6% of all mental health disabilities.
Why Veterans Get Mental Health Ratings Wrong
A mental health diagnosis alone is not enough. You must explain impairment.
How does it affect your work?
How does it affect your marriage?
How does it affect your kids?
How does it affect your sleep?
How does it affect your anger, anxiety, memory, motivation, mood, isolation, or ability to function?
Veterans are trained to suck it up. We minimize. We say, “Others had it worse.” We say, “I’m fine.”
But VA cannot rate what you refuse to say.
Tell the truth.
GWOT Veterans Have Some of the Most Complex Claims
The report also breaks out data for Global War on Terror veterans as a subset of the Gulf War Era.
VA reported 1,755,659 GWOT veterans receiving compensation.
Those veterans had 16,879,238 service-connected disabilities. That equals an average of 9.61 service-connected disabilities per GWOT veteran, which is higher than the overall average of 7.34.
Even more striking, 37.54% of all GWOT compensation recipients were rated 100%.
That is more than one out of every three GWOT veterans receiving VA compensation is rated at 100%.
This makes sense if you think about it.
Post-9/11 veterans often have complex claims involving deployments, airborne hazards, burn pits, chronic pain, joint injuries, blast exposure, mental health, migraines, sleep problems, respiratory issues, digestive issues, and secondary conditions.
For GWOT veterans, the top conditions included tinnitus, knee conditions, PTSD, back and neck strain, sciatic nerve issues, migraines, ankle conditions, scars, and allergic rhinitis.
Again, the lesson is simple: Complex claims require a strategy.
You cannot wing it.
Respiratory and Digestive Claims Are Rising
Another important trend in the report is the growth in respiratory and digestive conditions.
The report also showed respiratory disabilities among all compensation recipients increased 16.0% from FY2024 to FY2025.
Digestive disabilities increased 13.1%. Among new recipients, digestive disabilities increased 21.8%.
The report does not say every increase is because of the PACT Act, and we should not overstate that. But the trend is important.
Respiratory and digestive conditions are a major part of the modern VA claims landscape, especially for veterans with toxic exposure, burn pit exposure, Gulf War service, airborne hazards, sinus issues, rhinitis, asthma, sleep apnea, GERD, IBS, or related symptoms.
What Veterans Should Look At
If that is you, do not guess.
Look at your service history.
Look at your diagnoses.
Look at presumptive rules.
Look at secondary service connection.
Look at whether your current conditions may be connected to service or aggravated by another service-connected disability.
Female Veterans Had Higher 100% Rating Percentages
The report also shows an important trend for female veterans.
Among new female compensation recipients, 18.75% were rated 100%. Among new male compensation recipients, 15.00% were rated 100%.
Among all female compensation recipients, 32.55% were rated 100%. Among all male compensation recipients, 28.84% were rated 100%.
VA’s report does not explain why this gap exists, so we should be careful not to assume too much. But the data matters.
Female veterans should never assume their conditions “do not count” or that they are not eligible. They are.
Many female veterans have complex claims involving mental health, migraines, musculoskeletal conditions, reproductive health, military sexual trauma-related conditions, and other service-connected disabilities.
If you served and your condition is connected to service, you have the right to file. Period.
The Payment Gap Between 10% and 100% Is Life-Changing
The difference between 10% and 100% is not just a rating percentage. It can be life-changing money.
For new compensation recipients, VA reported the estimated average annual payment at 10% was $2,105. At 100%, it was $49,446.
For all compensation recipients, VA reported the estimated average annual payment at 10% was $2,122. At 100%, it was $50,793.
That’s a huge difference in compensation and benefits.
That is the difference between a couple thousand dollars per year and more than fifty thousand dollars per year in tax-free VA disability compensation.
Now, the goal is not to chase a rating you do not deserve. The goal is to make sure VA has the full and accurate picture of your service-connected disabilities.
Because if you are underrated, you could be leaving thousands of dollars in tax-free compensation on the table every single year.
What Veterans Should Do With This Data
Do not read this report and think, “Everyone should be 100%.” That is not true.
Read this report and think:
“I need to make sure VA has the full picture.”
That is the point.
Before you file a new claim, increase, supplemental claim, or higher-level review, ask yourself:
What conditions am I already service connected for?
Because a low rating does not always mean your condition is mild. Sometimes it means VA did not have the full picture. Sometimes it means you were underdocumented. Sometimes it means you missed secondary conditions. Sometimes it means you minimized your symptoms. Sometimes it means you did not explain functional impairment. Sometimes it means you need stronger evidence.
You served. You earned the right to file. You earned the right to be heard. And you earned the right to pursue every VA benefit you legally qualify for.
So here is the real question:
Do you have the VA rating you were given, or the VA rating you truly deserve?
Want Expert-Level VA Claim Help? WE GOT YOUR SIX!
VA Claims Insider helps educate and empower veterans to get the VA rating they deserve.
Work directly with a VA Claims Insider Coach who can help lead you to VA claim victory.
50,000+ disabled veterans served in our membership programs since 2016.
33% average rating increase for veterans who complete our #1 rated Elite program.
The Quality Assurance (QA) team at VA Claims Insider has extensive experience researching, fact-checking, and ensuring accuracy in all produced content. The QA team consists of individuals with specialized knowledge in the VA disability claims adjudication processes, laws and regulations, and they understand the needs of our target audience. Any changes or suggestions the QA team makes are thoroughly reviewed and incorporated into the content by our writers and creators.
Brian Reese is a world-renowned VA disability benefits expert and the #1 bestselling author of VA Claim Secrets and You Deserve It. Motivated by his own frustration with the VA claim process, Brian founded VA Claims Insider to help disabled veterans secure their VA disability compensation faster, regardless of their past struggles with the VA. Since 2013, he has positively impacted the lives of over 10 million military, veterans, and their families.
A former active-duty Air Force officer, Brian has extensive experience leading diverse teams in challenging international environments, including a combat tour in Afghanistan in 2011 supporting Operation ENDURING FREEDOM.
Brian is a Distinguished Graduate of Management from the United States Air Force Academy and earned his MBA from Oklahoma State University’s Spears School of Business, where he was a National Honor Scholar, ranking in the top 1% of his class.
BLUF: The VA doesn’t care how much evidence you submit; it cares whether the evidence proves your condition got worse.
The most important evidence for a VA rating increase is recent, credible medical and lay evidence showing your service-connected condition has worsened and now meets the criteria for a higher rating under the VA Schedule for Rating Disabilities (VASRD).
Many veterans believe they need to submit hundreds of pages of medical records to win an increased rating claim. That’s usually not true.
What matters most is whether your evidence clearly demonstrates worsening symptoms, greater functional impairment, and limitations that align with the next higher rating criteria. In many successful claims, the strongest evidence includes updated medical records, favorable C&P exam findings, DBQs, credible lay statements, and documentation showing how your condition affects work and daily life.
The key is quality and relevance, not volume.
Summary of Key Points
The best evidence for a VA rating increase directly matches the rating criteria for your condition under the VASRD.
Recent medical evidence showing worsening symptoms usually carries the most weight with VA raters.
DBQs, C&P exams, and objective findings can significantly strengthen your claim.
Lay statements and symptom journals help prove functional impairment and real-world limitations.
More evidence is not always better. Targeted, relevant evidence is more effective than overwhelming the VA with unnecessary records.
Table of Contents
Understanding VA Rating Increase Claims
A VA increased rating claim is for veterans whose service-connected disability has worsened since their last evaluation.
To approve a higher rating, the VA must see evidence that your condition now meets the criteria for the next higher percentage under the VA Schedule for Rating Disabilities (38 CFR Part 4). That means the VA is evaluating symptom severity, frequency, duration, functional loss, occupational impairment, and, in some cases, objective medical findings.
For example, migraine ratings often depend on the frequency of prostrating attacks and their impact on employability, while PTSD ratings focus heavily on occupational and social impairment. Orthopedic conditions may rely on range-of-motion measurements, flare-ups, and documented functional loss.
The strongest evidence specifically addresses the criteria required for the next higher evaluation.
What Evidence Matters Most for a VA Rating Increase?
1. Recent Medical Records Showing Your Condition Has Worsened
Current medical evidence is often the foundation of a successful VA increase claim.
The VA generally gives the most weight to recent treatment records showing symptom progression over time, failed treatments, worsening pain, increased medication usage, reduced functionality, or occupational impairment.
Strong evidence may include:
Specialist evaluations
Imaging results
Mental health treatment notes
Physical therapy records
Documentation of emergency care and hospitalizations
The strongest medical evidence is recent, specific, consistent over time, and supported by objective findings whenever possible.
The more clearly your records explain functional limitations, the stronger your claim becomes.
2. A Favorable C&P Exam Can Make or Break Your Claim
In many increased rating claims, the compensation and pension (C&P) exam becomes the single most influential piece of evidence.
Why? Because the examiner is specifically evaluating whether your symptoms meet the criteria for a higher rating.
A strong C&P exam may document reduced range of motion, pain during flare-ups, migraine frequency, occupational impairment, mental health symptoms, radiculopathy, or other findings that support a higher evaluation.
During your exam, be honest and accurate about how your condition affects you on your worst days. Explain how often flare-ups occur, how long they last, and what activities become difficult or impossible during those periods. Never exaggerate symptoms, but you shouldn’t downplay them either.
Whenever possible, submit strong medical evidence before your C&P exam. The examiner and rater will often compare your exam findings against the medical records already in your file.
DBQs are one of the most valuable tools available for a VA rating increase because they are designed specifically around the criteria VA raters use to evaluate disabilities.
A strong DBQ can:
Clarify symptom severity
Document flare-ups and functional loss
Capture occupational impairment
Directly address the criteria required for a higher rating
Because DBQs organize information in a format VA raters already understand, they can make it easier for the VA to identify qualifying symptoms and compare your condition against the VASRD.
Submitting a private DBQ doesn’t guarantee that the VA will skip a C&P exam. The VA still schedules additional exams frequently, even in well-supported claims.
4. Objective Medical Evidence and Specialist Opinions
Objective medical findings often carry significant weight because they provide measurable evidence of worsening.
Depending on your condition, this may include:
MRI findings
Reduced range of motion
Pulmonary function testing
Neurological evaluations
Cognitive testing
Sleep studies
EMG results
Specialist opinions can also be extremely persuasive in complex claims. For example, a neurologist may provide insight into migraine severity, while a psychiatrist or psychologist may document occupational and social impairment related to PTSD.
In some cases, an Independent Medical Opinion (IMO) can help address disputed C&P findings or explain why your symptoms satisfy higher rating criteria. The strongest IMOs clearly explain the severity of symptoms, the resulting functional impairment, and how the evidence supports a higher evaluation under the law.
5. Lay Statements and Buddy Letters
Lay evidence can be extremely powerful, especially for symptoms that are difficult to measure objectively.
The VA must consider competent lay evidence under federal law, and these statements often help fill in the gaps left by medical records.
Lay statements may come from:
You
Your spouse
Family members
Friends
Coworkers
Supervisors
The most effective statements are specific, detailed, and focused on observable limitations. A weak statement simply says a condition has worsened. A stronger statement explains exactly how symptoms affect daily life, employment, relationships, sleep, mobility, concentration, or social functioning.
For example, a spouse describing panic attacks, isolation, anger outbursts, or severe sleep problems can provide important context that may not fully appear in treatment notes.
The VA applies ratings based on diagnoses and impairment. Evidence showing reduced functioning in real-world situations can be critical for securing a higher evaluation.
These records help establish consistency over time and can support both medical evidence and lay statements.
A strong symptom log may track:
Frequency and severity of symptoms
Duration of flare-ups
Missed work
Medication use
Recovery time
Activities impacted by symptoms
Consistency matters more than perfection. Even simple notes documenting recurring limitations can help demonstrate the real-world impact of your condition.
Can Too Much Evidence Hurt a VA Rating Increase Claim?
Yes, sometimes.
One of the biggest mistakes veterans make is submitting massive amounts of irrelevant evidence in an attempt to strengthen their claim.
More evidence does not guarantee a better outcome.
Submitting hundreds of unrelated pages can slow processing, bury your strongest evidence, create inconsistencies, and make it harder for raters to identify the symptoms that actually support a higher evaluation.
Targeted evidence tied directly to worsening symptoms and rating criteria is usually more effective than volume.
Common Mistakes Veterans Make in VA Increase Claims
Submitting Outdated Medical Evidence
Older records may help establish medical history, but recent evidence usually matters most in increased rating claims.
If you haven’t sought treatment recently, the VA may conclude your condition has not significantly worsened. When possible, submit records from the past 6–12 months that clearly document increased severity and functional limitations.
Not Understanding the Rating Criteria
One of the most common reasons veterans lose increase claims is because their evidence does not match the legal criteria for the next higher rating.
Before filing, review your diagnostic code and understand exactly what symptoms, limitations, or occupational impairment the VA requires for a higher evaluation.
Downplaying Symptoms
Many veterans minimize symptoms during medical appointments or C&P exams because they are used to “pushing through.”
Unfortunately, that mindset can weaken a claim.
Be honest about pain levels, flare-ups, missed work, mental health symptoms, and daily limitations. The VA can only evaluate the symptoms and impairment that are documented in your records and examinations.
Does the VA Need New Evidence for a Rating Increase?
Yes, usually.
The VA generally expects evidence showing that your condition has worsened since your initial rating.
Updated treatment records, specialist evaluations, DBQs, imaging, worsening symptoms, or new C&P findings can all help support an increase claim.
How Much Evidence Is “Enough” for a VA Rating Increase?
There’s no specific number of records required.
Some veterans win increased ratings with a strong C&P exam, updated treatment records, and one detailed lay statement. Others may need more extensive evidence for complex conditions.
The goal is not to submit the most evidence but the right evidence, meaning it’s relevant, credible, recent, consistent, and directly connected to the rating criteria.
When Should You File for a VA Rating Increase?
Timely filling matters.
You should consider filing when your symptoms have clearly worsened, your condition causes greater functional impairment, or medical evidence supports a higher evaluation.
In most cases, the effective date for an increased rating is tied to either the date the VA receives your claim or the date evidence shows worsening occurred.
The strongest evidence for a VA rating increase is evidence that clearly proves your condition has worsened and now meets the criteria for a higher evaluation under the law.
For most veterans, that means recent medical records, favorable C&P exam findings, strong DBQs, objective testing, credible lay statements, symptom journals, and documentation showing occupational and functional impairment.
Remember: VA raters are comparing your symptoms against specific legal criteria, not simply counting pages of medical records.
The more directly your evidence supports those criteria, the stronger your claim becomes.
About VA Claims Insider
VA Claims Insider is the #1 most trusted name in VA disability claims.
Work directly with a VA claims coach who can educate throughout the claims process.
52,000+ disabled veterans have served in our membership programs since 2016.
33% average rating increase for veterans who complete our #1-rated Elite program.
What is the best evidence for a VA rating increase?
The strongest evidence usually includes recent medical records, favorable C&P exam findings, DBQs, objective testing, and credible lay statements showing worsening symptoms and functional impairment.
Do I need new medical evidence for a VA increase claim?
Usually, yes. The VA generally requires updated evidence showing your service-connected condition has worsened since your current rating was assigned.
Are DBQs important for a VA rating increase?
Yes. DBQs are specifically designed to document the symptoms and limitations VA raters use to evaluate disabilities under the VASRD.
Can lay statements help increase my VA disability rating?
Absolutely. Lay statements can provide valuable evidence about symptom severity, daily limitations, occupational impairment, and social functioning.
Can too much evidence hurt a VA claim?
Sometimes. Submitting excessive irrelevant evidence can bury the strongest parts of your claim and make it harder for raters to identify qualifying symptoms.
What if my C&P exam conflicts with my medical records?
The VA must weigh all evidence together. Strong treatment records, DBQs, or specialist opinions may help challenge unfavorable exam findings.
How recent should medical evidence be for a VA increase claim?
Generally, records from the past 6 to 12 months carry the most weight because they best reflect your current level of disability.
What form do I use to file for a VA rating increase?
Most veterans use VA Form 21-526EZ to request an increased disability rating.
About the Author
Katie McCarthy
Katie McCarthy is a writer and editor with experience in daily news and digital and print magazine publishing. She honed her editorial (and firearms) skills at Guns & Ammo before helping launch Black Rifle Coffee Company’s Coffee or Die Magazine as the managing editor. She holds degrees in English (BA) and public administration (MPA). Katie is a military spouse and word nerd who enjoys reading, hiking, camping, gardening, and spending time with her family.
2027 VA disability pay rates are projected to increase by 3.9% with the annual COLA. If that estimate holds, it would be the largest COLA increase for veterans since 2022.
But here’s the deal: These rates are not official yet. The final 2027 COLA won’t be announced until mid-October 2026, after the July, August, and September CPI-W inflation data is released.
For now, we’ve applied a projected 3.9% COLA to the official 2026 VA disability rates so you can estimate your projected 2027 tax-free monthly VA compensation by rating and dependents.
2027 VA Disability Pay Rates (Without Children)
Rating
Veteran Alone
Veteran & Spouse
Veteran, Spouse, & One Parent
Veteran, Spouse, & Two Parents
Veteran & One Parent
Veteran & Two Parents
100%
$4,092.18
$4,320.34
$4,503.45
$4,686.57
$4,275.30
$4,458.41
90%
$2,454.43
$2,659.15
$2,823.37
$2,987.59
$2,618.65
$2,782.87
80%
$2,184.13
$2,365.71
$2,512.03
$2,658.36
$2,330.46
$2,476.79
70%
$1,878.98
$2,038.12
$2,166.29
$2,294.47
$2,007.15
$2,135.32
60%
$1,490.99
$1,627.70
$1,736.65
$1,845.59
$1,599.92
$1,708.87
50%
$1,177.08
$1,290.30
$1,381.09
$1,471.88
$1,267.87
$1,358.66
40%
$826.88
$917.67
$990.29
$1,062.92
$899.50
$972.13
30%
$574.02
$642.37
$696.85
$751.32
$628.49
$682.96
Rating
100%
90%
80%
70%
60%
50%
40%
30%
Additional For A/A Spouses
$209.26
$187.99
$167.69
$146.33
$124.97
$104.67
$83.31
$61.95
2027 VA Disability Pay Rates (With Children)
Rating
Veteran & Child
Veteran, Spouse, & Child
Veteran, Spouse, Child, & One Parent
Veteran, Spouse, Child, & Two Parents
Veteran, Child, & One Parent
Veteran, Child, & Two Parents
100%
$4,244.76
$4,487.43
$4,670.55
$4,853.67
$4,427.88
$4,610.99
90%
$2,591.16
$2,810.11
$2,974.64
$3,139.08
$2,755.61
$2,920.13
80%
$2,305.90
$2,500.28
$2,646.62
$2,792.96
$2,452.23
$2,598.56
70%
$1,984.72
$2,155.62
$2,283.79
$2,411.97
$2,112.89
$2,241.07
60%
$1,581.78
$1,728.11
$1,837.06
$1,946.00
$1,690.71
$1,799.66
50%
$1,252.92
$1,374.68
$1,465.47
$1,556.26
$1,343.71
$1,434.50
40%
$887.76
$984.95
$1,057.57
$1,130.20
$960.38
$1,033.01
30%
$618.88
$692.59
$747.06
$801.54
$673.35
$727.83
Rating
100%
90%
80%
70%
60%
50%
40%
30%
Each Additional Child Under 18
$113.37
$101.47
$89.72
$79.04
$67.29
$56.60
$44.86
$33.11
Each Additional Schoolchild Over 18
$366.20
$328.97
$292.66
$255.27
$218.96
$182.65
$146.33
$108.95
Frequently Asked Questions
What is the 2027 COLA prediction?
The latest 2027 COLA prediction is 3.9%, according to The Senior Citizens League, with some estimates as high as 4.2% if inflation stays elevated. The official COLA won’t be announced until October 2026, after July, August, and September CPI-W data is released.
Why does the projected 2027 COLA keep increasing?
The projected 2027 COLA keeps rising because inflation is running hotter than expected. Everyday costs like energy, housing, food, utilities, and healthcare are still putting pressure on Americans, which is why COLA estimates have moved higher in recent months.
What is the projected 2027 VA disability pay increase?
The projected 2027 VA disability pay increase is 3.9%. If that estimate holds, veterans rated 10% or higher would see their tax-free monthly VA compensation increase beginning with their January 2027 payment. A 3.9% COLA boost would also be the largest COLA for veterans since 2022. For example, a veteran receiving $1,000/month in 2026 would see about a $39/month increase in 2027, while a veteran receiving $4,000/month would see about a $156/month increase.
When do the new rates take effect, and when will I see the higher payment?
The new 2027 VA disability pay rates will take effect on December 1, 2026. Because VA pays disability compensation in arrears, your December 2026 benefits are paid in your January 2027 payment. That means veterans should typically see the higher 2027 VA disability payment around January 1, 2027. However, your deposit may arrive one to three days early depending on your bank or credit union, including institutions like USAA or Navy Federal.
Do I need to do anything to get the 2027 COLA increase?
No. The COLA increase is automatic. You don’t need to apply, call the VA, or submit a claim. The VA adjusts your benefit amount internally based on your VA rating, and you’ll see the change reflected in your January 2026 deposit. If you’re receiving multiple VA benefits—like Special Monthly Compensation (SMC), Dependency and Indemnity Compensation (DIC), or VA Pension—they’ll all increase automatically as well.
Who gets the 2027 COLA increase?
All veterans with a VA disability rating of 10% or higher should qualify for the 2027 COLA increase if it’s finalized. That includes veterans rated from 10% to 100%, veterans receiving Total Disability Individual Unemployability (TDIU) paid at the 100% rate, and recipients of Special Monthly Compensation (SMC), Dependency and Indemnity Compensation (DIC), or VA Pension benefits. If you have a 0% VA rating, you won’t see a monthly pay increase because 0% ratings do not include monthly VA disability compensation.
Do I get extra dependent pay at 10% or 20%?
No. Veterans rated at 10% or 20% receive a flat monthly rate, regardless of dependents. Additional VA compensation for dependents, including a spouse, children, or dependent parents, starts at a combined VA disability rating of 30% or higher. See the projected 2027 VA pay tables above to estimate your monthly compensation with or without dependents.
Does the projected 2027 3.9% COLA affect my retroactive or back pay?
It depends on the months covered by your retroactive pay. VA back pay is calculated using the pay rates that were in effect for each month of your retro period. If your back pay includes months after December 1, 2026, those months would use the new 2027 VA disability rates. But if your back pay covers earlier years, those months are calculated using the VA pay rates in effect for those specific years.
Is VA disability pay taxable?
No. VA disability compensation is completely tax-free at both the federal and state levels. That includes payments for SMC, DIC, VA Pension, and Combat-Related Special Compensation (CRSC). If you receive both VA disability and military retired pay, make sure to review your DFAS Form 1099-R to understand which portions are taxable. See my full breakdown of Veterans’ Tax Rules and Exemptions.
How does the VA determine my disability rating?
The VA uses the Schedule for Rating Disabilities (VASRD) found in 38 CFR Part 4 to assign a percentage to each service-connected condition. Each condition gets a diagnostic code and rating level based on symptom severity, frequency, and impact on your work and life. If you have multiple service-connected conditions, VA applies the Combined Ratings Table—often called “VA math”—to determine your final combined rating. Try our free VA disability calculator to quickly find your combined VA rating and monthly payment amount.
Can I file for a VA disability rating increase?
Yes. If your service-connected conditions have worsened or you’ve obtained new medical evidence, you can request a VA rating increase at any time through VA.gov. A properly documented increase claim can often raise your monthly benefit more than a COLA adjustment alone. If you need help developing your evidence and strategy, see my guide: 8 Ways to Increase Your VA Disability Rating.
How do I find VA resources near me?
You can search for VA-accredited VSOs, attorneys, or claims agents using the VA’s official tool (VSO services on claims are free), and you can look up nearby VA facilities (medical centers, Vet Centers, regional benefits offices).
Want Expert-Level VA Claim Help? WE GOT YOUR SIX!
VA Claims Insider is the #1 most trusted name in VA disability claims.
Work directly with a VA Claims Insider Coach who can help lead you to VA claim victory.
50,000+ disabled veterans served in our membership programs since 2016.
33% average rating increase for veterans who complete our #1 rated Elite program.
The Quality Assurance (QA) team at VA Claims Insider has extensive experience researching, fact-checking, and ensuring accuracy in all produced content. The QA team consists of individuals with specialized knowledge in the VA disability claims adjudication processes, laws and regulations, and they understand the needs of our target audience. Any changes or suggestions the QA team makes are thoroughly reviewed and incorporated into the content by our writers and creators.
Brian Reese is a world-renowned VA disability benefits expert and the #1 bestselling author of VA Claim Secrets and You Deserve It. Motivated by his own frustration with the VA claim process, Brian founded VA Claims Insider to help disabled veterans secure their VA disability compensation faster, regardless of their past struggles with the VA. Since 2013, he has positively impacted the lives of over 10 million military, veterans, and their families.
A former active-duty Air Force officer, Brian has extensive experience leading diverse teams in challenging international environments, including a combat tour in Afghanistan in 2011 supporting Operation ENDURING FREEDOM.
Brian is a Distinguished Graduate of Management from the United States Air Force Academy and earned his MBA from Oklahoma State University’s Spears School of Business, where he was a National Honor Scholar, ranking in the top 1% of his class.




 Call us now at
Call us now at