The consulting firm Milliman recently published its 2025 Long-Term Care Index, calculating that – on average – 65-year-olds should set aside $135,000 for their future high-intensity long-term care needs.
Great Variability
While an average figure can be a helpful anchor point, Milliman’s estimates show substantial variability based on gender, location, and health status, among other factors. For instance, the average cost for women is $171,000 and that for men is $98,000, largely because women live longer. As a result, they may need care for a longer period of time and are less likely to have a spouse available to assist them at no cost.
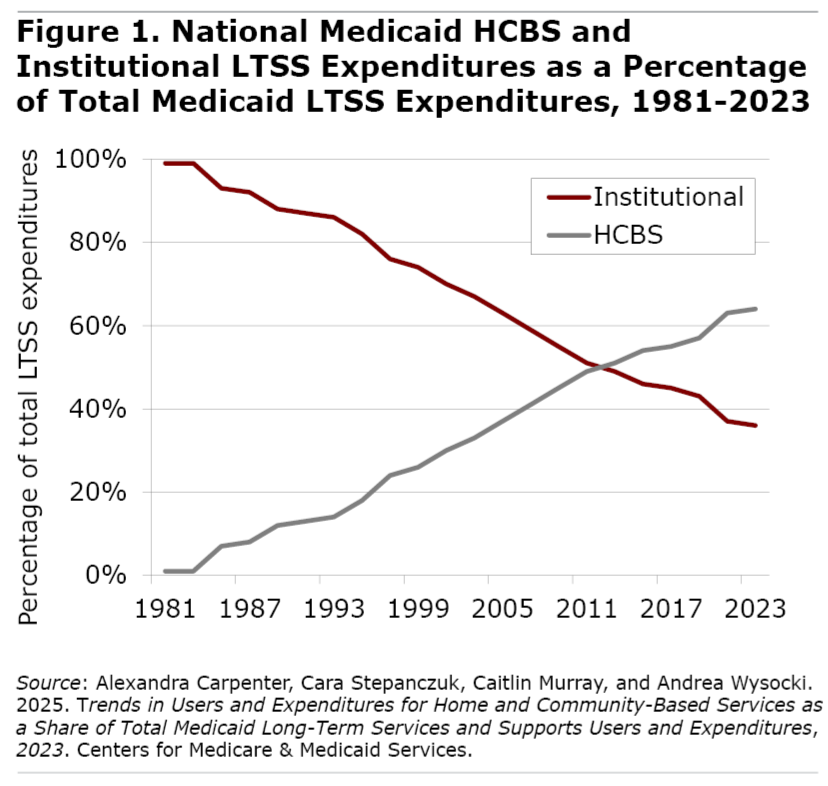
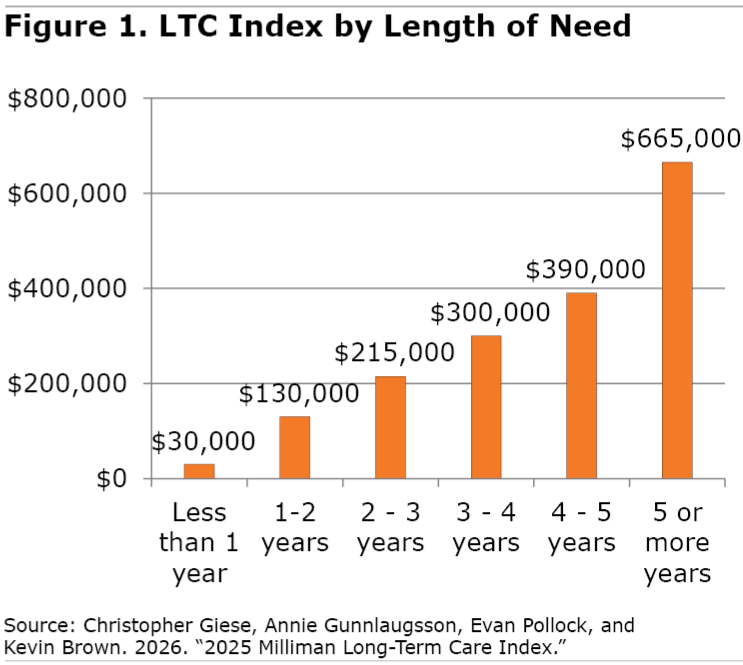
According to Milliman, almost half of men and four out of ten women will need no paid care at all during their lives. Another quarter of men will receive less than a year of paid care, leaving just 29 percent requiring more than a year of paid care. Women, on the other hand, are much more likely to need care for an extended period with 41 percent facing more than a year and 14 percent needing five years or more, which will on average cost them $665,000 (see Figure 1).
I should note that the Milliman figures assume all care is paid care. The Center for Retirement Research at Boston College has estimated that families typically provide at least half of the care hours, even for those with high needs. Milliman also doesn’t say how these costs are paid, in particular whether they include Medicaid-covered care or only amounts paid out-of-pocket.
Location, Location, Location
Costs vary considerably by type of care needed – home health, assisted living, or nursing home – and by location. Location matters not only in terms of costs of care but also longevity and health. People live longer (and, thus, may need care longer) in some states – such as Hawaii, California, Washington, Florida and New Hampshire – than others – such as Mississippi, Alabama, West Virginia, Louisiana and Kentucky.
On the other hand, people who are healthier tend to need care for less time. Milliman highlights Colorado, Montana and Hawaii as states where residents are least likely to need any paid long-term care and Montana, again, along with Arizona and Oklahoma as the states where people need the shortest duration of care. At the other end of the spectrum, those with care needs in Hawaii, Connecticut and New York receive care for the longest periods of time.
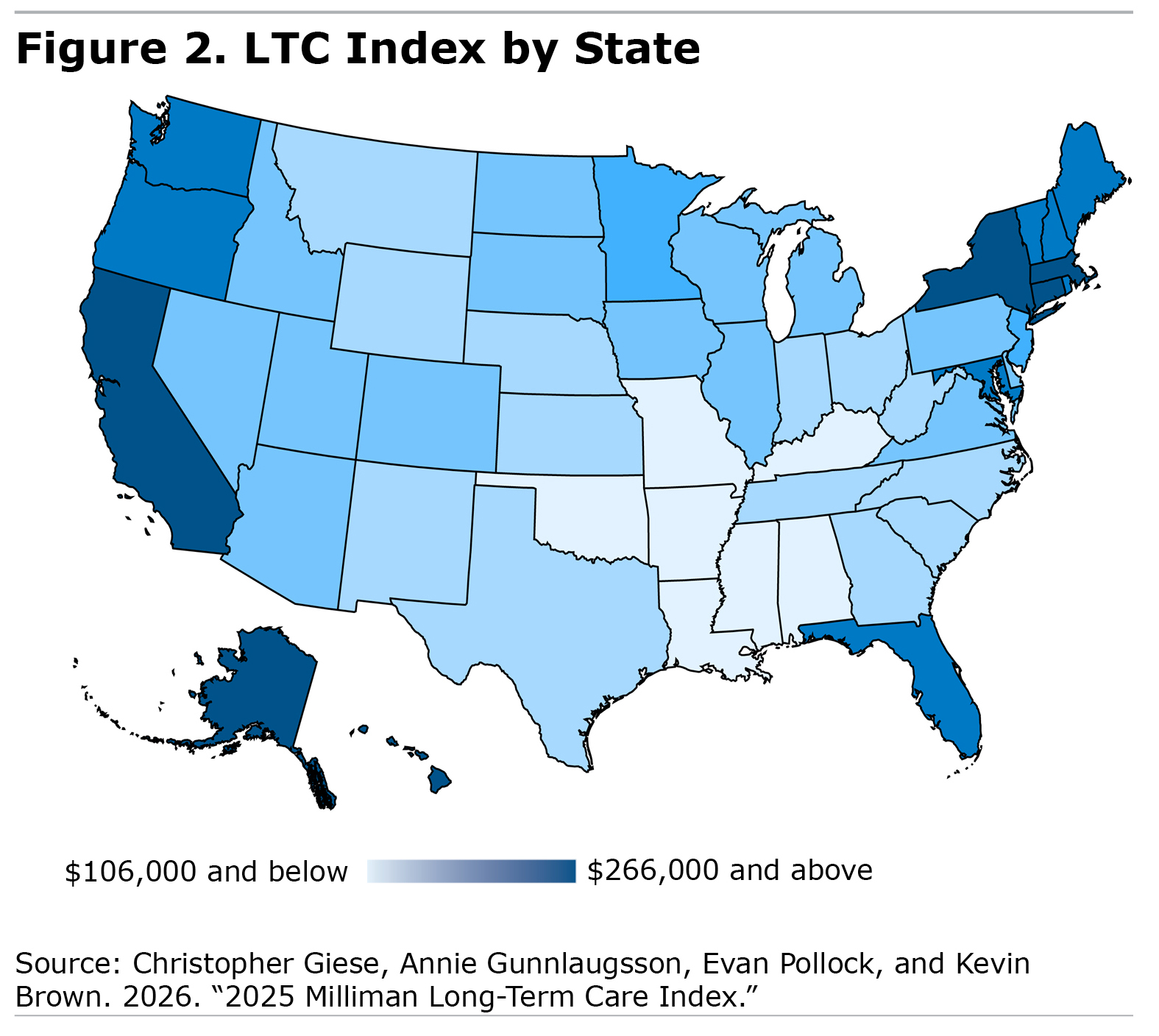
Combining all these factors – so that the cost of LTC services, the likelihood of needing services, and the duration of the needs are accounted for – Figure 2 shows Milliman’s ranking of the average long-term care costs per state (see Figure 2).
The most expensive states (dark blue) are on the West Coast and in the Northeast, where average costs are about twice the national average. The least expensive are largely in the South-Central region (light blue).
A further variation on how much 65-year-olds need to set aside for their care is the anticipated rate of return. The $135,000 average is based on an average investment return of 4.35 percent. Using a higher figure of 7 percent, the average 65-year-old would only need to set aside $74,000, but using a lower return of 3 percent, they’d need $187,000 in the bank.
What Does This Mean for You?
For individuals and families planning for future long-term care costs, it can be difficult to anticipate the need. I’ve written before about the factors that affect the need for paid long-term care, including overall health, family history, and family situation.
But the $135,000 figure seems like a good starting point. Increase that number if you live in a high-cost state, have a family history of dementia or other illnesses that may require a long period of assistance, or if you do not have family members who could help.
Your existing health may affect the figure both positively and negatively. If you are already suffering from a debilitating chronic disease that you could live with for many years, such as Parkinson’s, you can anticipate needing more money. But if you have a form of cancer that may shorten your life but not lead to a long period of disability, you may need considerably less.
An Insurance Solution?
My biggest take away from the Milliman report is that we need a universal long-term care insurance program since we have great uncertainty about individual needs combined with relative certainty about those of the entire elder population. In addition, while a small minority of seniors can afford the cost of their care, whatever it may be, a majority cannot.
According to the Federal Reserve, the median retirement savings of 65- to 74-year-olds in the United States is $200,000, meaning that half have less than this amount. Individuals ages 75+ have median savings of just $130,000. In short, most baby boomers likely do not have enough money to pay their future long-term care costs.
The cost for covering long-term care needs would be significantly less if we started contributing at an earlier age through a national insurance plan. At its 4.35-percent rate of return, Milliman calculates a 35-year-old would only have to set aside $38,000, on average, to cover their future long-term care costs, almost $100,000 less than a 65-year-old. Of course, few 35-year-olds are thinking about their future care needs, but collectively we can approach this challenge. In fact, Washington State has set up such a program, which provides a base layer of long-term care protection for its workers (up to $36,500); and it is exploring ways to allow people to buy additional long-term care insurance at a group rate. Several other states, including Massachusetts, are already exploring similar programs.
For more from Harry Margolis, check out his Risking Old Age in America blog and podcast. He also answers consumer estate planning questions at AskHarry.info. To stay current on the Squared Away blog, join our free email list.