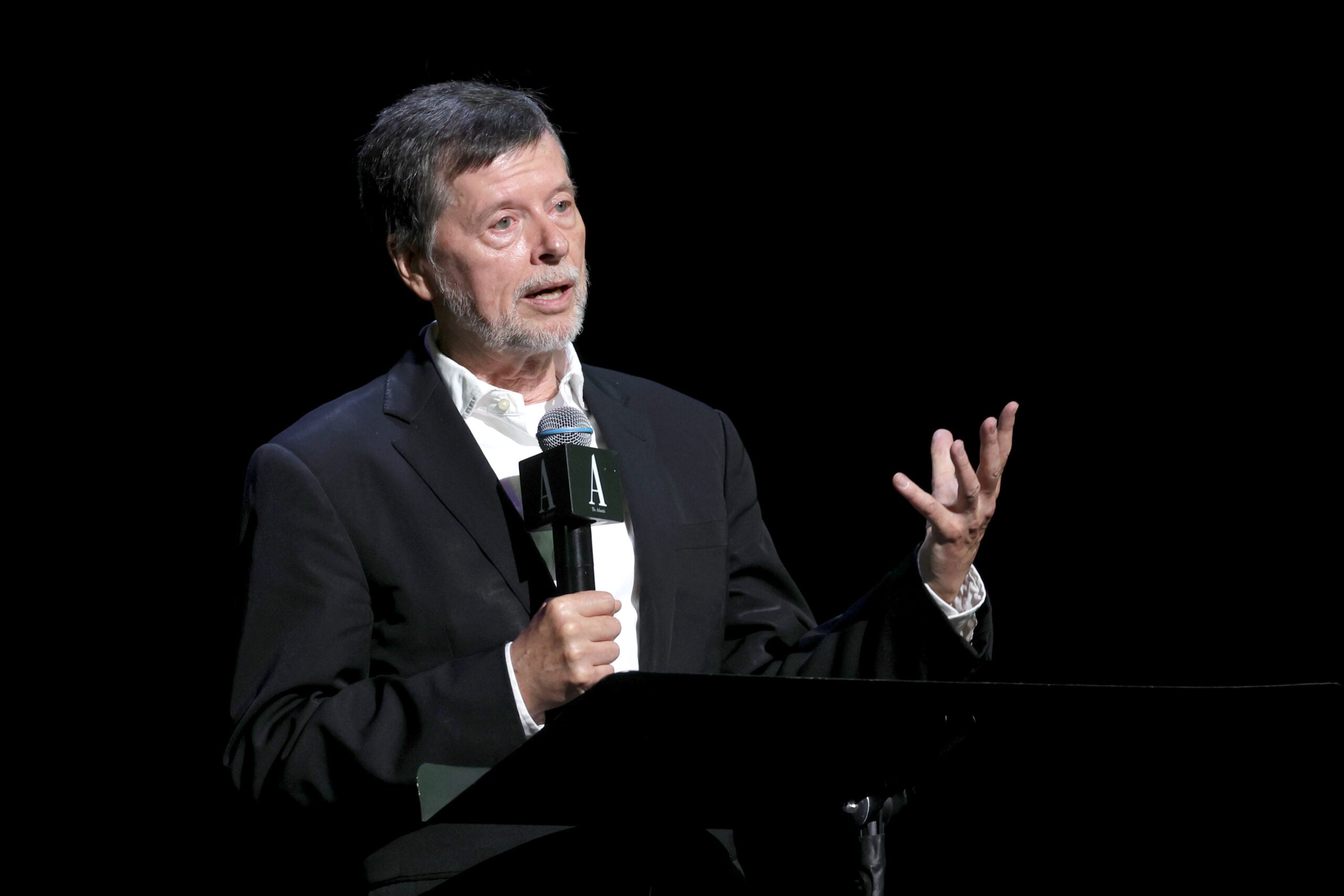
Ken Burns has had a busy year.
The famed documentary filmmaker and his co-producers, Sarah Botstein and David Schmidt, have stumped across the United States, speaking, gently of course, about their upcoming docuseries, “American Revolution,” which premieres Sunday on PBS.
During their six-month promotional tour across 32 cities and 17 states, the trio has consistently delivered a nonpartisan, hopeful message to Americans.
“We think always in sort of Chicken Little terms,” Burns told an audience during a panel event at Mount Vernon, Virginia, on Oct. 29, “that our time must be the very, very worst.”
“You can have at least the possible reassurance that things were really divided back then. It was a civil war,” he said of the American Revolution. “Examining the origin story provides you with a kind of renewal and a fresh understanding.”
Burns has endeavored to provide such reassurances. The director and his team have spoken to a spectrum of media over the course of the year, from podcasters like Theo Von and Joe Rogan to MSNBC and The New York Times.
Burns spent nearly two hours on Von’s show and three on Rogan’s, with one listener noting in the latter’s YouTube comment section, “We need an annual Ken Burns discussion, if not more. This is cathartic.”
“We’re trying to reach as many people as we can,” Schmidt told Military Times in a recent interview. “If anybody wants to talk to us, we’re really happy to speak to them.”
The makings of liberty
For Burns and his team, the decision to make a documentary on the American Revolution was “spontaneous,” according to the director.
To put it into context, the year was 2015, President Barack Obama still had 13 months left in his presidency and “nobody was talking 250” — America’s semiquincentennial anniversary in 2026 — Burns told the audience at Mount Vernon.
“But I was looking at this map that we had of the Ia Drang Valley, in the central highlands [of Vietnam], and I just said, ‘That could be the British moving west on Long Island towards American positions in Brooklyn,” Burns recalled at the Mount Vernon panel. “I just went, ‘We could do it.’”

The filmmakers, however, had to get creative. Without photographs, B-roll or archival footage, the trio resorted to maps, diaries and reenactors to tell the epic tale of Great Britain’s 13 North American colonies’ fight for independence.
“We went out and filmed with reenactors,” Schmidt said of the filmmaking process, which also included commissioning watercolors from a group called Wood Ronsaville Harlin.
“Probably the most expensive line item in our budget is re-creating North America as faithfully as we could in a map,” he noted. “That was challenging, but also really fun. Waterways across America have changed since the 18th century. We had to erase the Erie Canal. Stuff like that you just don’t think of.”
Despite such challenges, according to Schmidt, the lack of visual primary sources presented opportunities to find “new ways to solve these problems.”
Over the course of several years, the trio shot original footage of nearly 100 locations within the original 13 colonies, as well as in London and the English countryside.
For 10 years — and to the tune of more than $30 million — Burns and his team built up a vast archive of knowledge.
“Part of the reason it was so exciting to make [this film] is that we got to spend a decade learning what actually happened and finding out the way to artistically shape that into a 12-hour film to share with the American people,” Schmidt shared.
“We aren’t trying to dispel myths. We’re not mythbusters out there poking holes in your understanding of the American Revolution. In fact, what we’re doing is taking what you already know and rebooting it,” he said. “It’s going to supplement what you already know and make it make more sense.”
Heart of the story
The six-part series follows more than just the well-known characters of the American Revolution.
While it includes rank-and-file Continental soldiers, militiamen and American Loyalists, the series also delves into the oft-unheard stories of Indigenous soldiers and civilians, enslaved and free African Americans, German soldiers in the British service, French and Spanish allies and an array of civilians living in North America.
The documentary highlights a war that not only touched the lives of those living within the 13 colonies, but also engaged and inspired millions of people in North America and beyond.

“The war begins in Lexington,” Schmidt said, “but it spreads all throughout — not just the original 13 colonies — but over the mountains to the Ohio River, along the Gulf Coast, even out to the Mississippi River. It’s also in the Caribbean. It’s fought off the coast of England. It’s fought in the Atlantic Ocean. It’s fought along the coast of France, along the coast of Africa, even in the Indian subcontinent — and that’s just the war.
“The ideas just grow and grow and inspire revolutions — and have inspired revolutions for the past 250 years all throughout the world. Ho Chi Minh, when he declared Vietnamese independence, had two United States OSS officers standing next to him and was quoting Thomas Jefferson in Vietnamese.”
Despite these ideas that have shaped the world since 1776 (many argue that date is even earlier), Schmidt recalls how surprised he was when learning about the original aims of the conflict.
The now-lauded notions of civilian rule and non-partisanship that created the republic that we still live under were not, says Schmidt, “on the table at the start.”
“Those weren’t war objectives,” he continued. “On April 19, 1775, they became necessary to win the war. But they were kind of outcomes of the war, rather than goals. What they were really trying to do at the start was to liberate Boston, to get a redress of grievances and to bring things back to the way they were under the British Empire. But in order to win the war, they had to involve all sorts of American people who otherwise might not get along.
“Coalition building made it a war about liberty. It made it this fight for a union. Then in order to win the war, they had to involve foreign powers. The French came in. The Spanish came in as the allies of the French. The Dutch declared war on the British,” ultimately creating a coalition war.
Former Commandant of the Marine Corps Gen. Joseph Dunford, who spoke alongside Burns at the panel at Mount Vernon, echoed Schmidt.
“I would argue — and I think it’d be tough to argue against it — that our strategic center of gravity as a country comes from allies and partners,” Dunford said. “There’s almost nothing that we have to deal with, certainly in the 21st century, where coherent collective action isn’t required to address a problem.”
That coalition is what makes up the heart of the documentary. Nearly 150 characters are highlighted in the series, with their stories read by a staggering 61 different voice actors, including: Kenneth Branagh, Josh Brolin, Jeff Daniels, Morgan Freeman, Paul Giamatti, Domhnall Gleeson, Tom Hanks, Ethan Hawke, Samuel L. Jackson, Michael Keaton, Damian Lewis, Laura Linney, Edward Norton, Mandy Patinkin and Meryl Streep, among many others.
The military story itself features 36 battle sequences that range from the well-known, like Bunker Hill and Yorktown, to the more obscure, while showing that the American Revolution was a test of logistics and strategy as much as it was a war of ideals.

George Washington is, naturally, also front and center in the series — a point that Burns noted while speaking at the historic home of America’s first president.
“He’s our guy, and that’s pretty amazing. Look, we do not soft pedal the flaws. Not only are there really bad tactical mistakes: there’s the rashness of riding out on the battlefield, not just as Princeton but at Monmouth and Kip’s Bay; and he owns hundreds of human beings. You can’t square that circle. But we are so lucky [to have had him], and we’re here because of him.”
Civilians, not subjects
One point that Burns and his team spend considerable time exploring is the notion of citizenship.
“I’m really still overwhelmed by some of the obvious things, that for the first time, we were creating citizens, not subjects under authoritarian rule,” says Burns.
“Thomas Jefferson says, ‘All experience has shown that mankind are more disposed to suffer while evils are sufferable.’ That just means that for most of human history, people have been under authoritarian rule and they’ve accepted it. They’ve acquiesced that those evils are sufferable. Essentially this [American] ‘project’ was to say no to that.”
The war, however violent and bloody it was (which Burns succeeds in displaying) was the vehicle for that freedom.
“I’m really proud to have worked on this film. I’m prouder to be a citizen of a country that invented that idea,” he added.
Burns ended the panel with a potent mix of patriotism grounded in history, closing with one of his favorite quotes from a Hessian soldier, Johann Ewald, who served under the British during the war.
“Who would have thought 100 years ago that out of this multitude of rabble would arise a people who could defy kings?” Ewald once quipped.
“That to me,” says Burns, “is the whole essence of the project. The right to defy kings.”










{kind=link}
{kind=link}